Download
1 / 21
240 likes | 722 Views
Overview of Allergy Testing. Author:???? Editor: Amy Shaheen, MD, Assistant Professor of Clinical Medicine Duke University Medical Center. Allergic Rhinitis — Basic Principles: Epidemiology. Epidemiology .

E N D
Overview of Allergy Testing Author:???? Editor: Amy Shaheen, MD, Assistant Professor of Clinical Medicine Duke University Medical Center
Allergic Rhinitis — Basic Principles: Epidemiology • Epidemiology. • Allergic rhinitis (AR) is one of the most prevalent diseases, affecting approximately 10-30% of all adults. The morbidity associated with AR is manifested through lost work and productivity, as well as an increasingly well-documented link between AR and the development of asthma. The “one airway” hypothesis has shown that inflammation in rhinitis is associated with inflammation of the lower airways, as seen in asthma.
Allergic Rhinitis — Basic Principles: History & Physical Exam • History & Physical Exam • Physical findings • “Allergic shiners”, which are dark circles around the eyes from persistent rubbing • “Allergic salute” is a horizontal crease in the skin over the juncture of nasal septal cartilage and bone, resulting from constant wiping of the nose in childhood. • The nasopharynx is classically pale and edematous in AR. • Nasal exam is important to exclude polyps, obstructing lesions, or purulent mucous, any of which might suggest other causes of symptoms
Allergic Rhinitis — Basic Principles: Differential Diagnosis • Differential diagnosis. • Other causes of similar symptoms include infectious rhinitis, nasal polyps, vasomotor rhinitis, gustatory rhinitis, hormonally influenced rhinitis (i.e., hypothyroidism or pregnancy), tumor, NARES (non-allergic rhinitis with eosinophilia syndrome), and drug-induced rhinitis (i.e., rhinitis medicamentosa secondary to overuse of topical decongestants, or side effects from medications including Aspirin, ACE
Allergic Rhinitis — Basic Principles: Classification of AR symptoms Classification of AR symptoms. Formerly, AR was described as seasonal or perennial, based on whether symptoms occur intermittently or throughout the year. More recently, it has been proposed to change the classification to intermittent or persistent. The WHO guidelines for classifying AR are as follows:
Allergic Rhinitis — Basic Principles After using the history and physical exam to make a presumptive diagnosis of AR, the next step in its management is usually a therapeutic trial Given the extremely high prevalence of AR, and the minimal adverse effects from medications to treat it, treating AR presumptively is a generally followed practice supported by guidelines.
Allergic Rhinitis — Treatment of AR a.Treatment of AR. Available medications to treat AR act to thwart the pathologic response to allergen.
Allergic Rhinitis — Allergen Avoidance & Antihistamines • Allergen avoidance. • Although clearly helpful in easily identified allergic triggers such as pets, some evidence suggests that commonly recommended practices such as dust covers for mattresses are not helpful in reducing AR symptoms (Terreehorst et al, N Engl J Med. 2003 Jul 17;349(3):237-46). Barring further evidence, the recommendations have been to wash bedsheets weekly in hot water, avoid or remove carpets in homes, and minimize exposure to pets if a patient suffers from indoor allergies. • Antiihistamines • act by blocking the H1 receptor to decrease histamine-mediated symptoms such as sneezing, itchy eyes, and rhinorrhea (i.e., early response symptoms). They are not effective for treating nasal congestion. Nonsedating antihistamines include fexofenadine, loratadine, and cetirizine. Even these agents can have a sedating effect, with fexofenadine having the least propensity to induce drowsiness.
Allergic Rhinitis — Topicals and Nasal cromolyn • Topical corticosteroidssuch as flunisolide reduce inflammation in the nasopharynx, and relieve symptoms of congestion. They are not effective for itchy eyes. Patients intolerant to aerosolized topical corticosteroids may be able to use aqueous solutions instead. • Topical opthalmic preparations such as Patanol are effective for red or persistently itchy eyes. • Nasal cromolyn acts to stabilize mast cells in the nasal mucosa, inhibiting the release of histamine and improving symptoms. The frequent dosing necessary for effect (3 or more times per day) makes compliance more difficult.
Allergic Rhinitis — Allergen Immunotherapy • Allergen immunotherapy consists of a series of allergen “shots” in increasing doses to alter the immune response to specific allergens. The theoretical basis is that the Th2 immune response (i.e., IgE-mediated response with prominent eosinophilia, IL-4, IL-5, and IL-13) is shifted to a Th1 response (characterized by TNF-alpha, IFN-gamma, IL-1). Before undergoing allergen immunotherapy, a patient must be identified as having IgE responses to specific allergens.
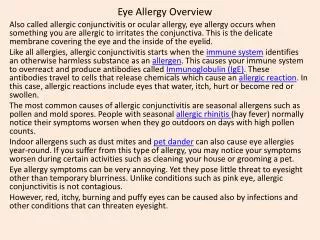
Allergy Testing: Indications for allergy testing • Allergy Testing • As seen in the previous slide, there are multiple therapeutic options to treat AR empirically prior to the identification of specific allergens. Allergy testing in the setting of AR identifies IgE antibodies to a particular antigen that may be triggering a pathologic response, leading to symptoms. • Indications for allergy testing: • Failure of initial medical therapy • Need to confirm the diagnosis of allergic rhinitis • Plan to pursue allergen immunotherapy
Skin Testing • Priniciples: Skin testing involves introduction of an allergen into the skin to provoke an IgE-mediated response that correlates with allergic triggers of AR. • Techniques: Two types of skin testing (Figure 1) are: • Puncture testing. In this technique, a small needle is dipped in a standardized allergen solution, then applied to the skin with a prick that breaks the epidermis but does not draw blood or pierce the dermis. • Intradermal testing Intradermal testing is essentially similar to PPD testing for TB in technique, where a small amount of allergen is injected into the dermis. • Puncture testing is slightly less sensitive than intradermal testing, but intradermal testing is associated with a 0.02% to 0.04% risk of moderate to severe adverse reaction, such as urticaria.
Allergy Testing: Controls & Allergen Selection • Controls & Allergen Selection • Skin tests use positive and negative controls to ensure accuracy of the results. The positive control is histamine, which induces a “wheal and flare” reaction. The negative control is the diluent solution for the allergens. The allergens tested usually include a panel of several (up to dozens) of standardized compounds that are derived from outdoor allergens such as grasses, trees, and pollens, and indoor allergens such as dust mite, animal dander, and molds. The specific allergens used vary by geographic location (i.e., the grasses and trees in North Carolina differ from those in Oregon, and necessitate testing for different allergens).
Allergy Testing: Causes of inaccurate results & precautions • Causes of inaccurate results and precautions. Factors affecting reaction to positive control (and subsequent allergy testing results) include: • Dermographism. Patients who have a wheal-and-flare reaction to simple scratching of the skin will have false positive results. • Age. Greater age correlates with reduced skin test reactivity • Use of rx such as antihistamines, topical corticosteroids, clonidine, tricyclic antidepressants, or phenothiazines. These medications will blunt the skin response, and either should be discontinued 10 days prior to skin testing, or patients on these medications should undergo alternate means of allergy testing. • Patients on beta blockers and ACE inhibitors. These patients should not undergo allergy testing unless it is possible to discontinue the medication temporarily for the test, as these medications will interfere with the rare need to treat adverse systemic reactions, such as urticaria/angioedema.
Allergy Testing: Common methods of allergy skin testing Figure 1:Common Methods for allergy skin testing
Allergy Testing: Interpretation & Accuracy • Interpretation of results • The degree of wheal (induration) and flare (erythema) response is assessed at the time of maximal IgE-mediated response (about 15-20 minutes) to determine whether there is a specific IgE response to a given allergen. The wheal is measured and given a semi-quantitative value. A positive result must be interpreted with the patient’s symptoms to determine whether an allergen is a true trigger of symptoms. Positive results for specific allergens confirm the diagnosis of allergic rhinitis and, if necessary, guide the formulation of specific allergen immunotherapy. • Accuracy of Skin Test Results. • The sensitivity of puncture skin tests range from 90-95% in most studies, and specificity is from 80-90% in most studies1. Skin test results must be interpreted in the context of the patient’s symptoms.
In Vitro Allergy Testing (RAST) • Principles and Techniques. - in vitro allergy testing is based on detecting specific IgE in the blood that recognizes allergens likely to cause symptoms of AR. The most commonly used test is RAST (radioallergosorbent testing). In this test, allergen is bound to a cellulose disk, and serum added to the disk. Specific IgE in the serum binds to the allergen, and subsequently detected using radioisotope-tagged anti-human IgE antibodies. The amount of specific IgE can be detected this way. **Note that measurement of serum total IgE is not a useful test in the diagnosis of allergic rhinitis, as it is neither sensitive nor specific** • Interpretation of Results. RAST testing is not as sensitive as skin testing in detecting specific IgE responses. Part of the explanation for this is that it detects only IgE in the serum, whereas most IgE important for allergic responses is located in the peripheral tissue. However, one of the benefits of RAST is that patients on medications that contraindicate skin testing (i.e., beta blockers or TCA antidepressants) may still undergo allergy testing.
In Vitro Allergy Testing (RAST) - continued • Otherin vitro Techniques. There are more advanced tests such as multiallergen screening tests and tests for markers of basophil activation that are beyond the scope of this topic. • Accuracy of Results. The sensitivity of in vitro allergy testing ranges from 60-80% in most studies, and specificity ranges from 70-90% in most studies1.
Allergy Testing: Recommendations • Recommendations • The benefits of skin testing include lower cost, more specificity, and a functional measure of the IgE immune response. The benefits of in vitro allergy testing include lack of contraindication if a patient is on certain medications, albeit at more expense. Currently, the AAAAI, ACAAI, and ECAAI recommend either skin testing or in vitro testing as an initial approach to diagnosing allergic rhinitis. This is supported by a recent meta-analysis and review of allergy diagnostic testing1
Other indications for Allergy Testing • Penicillin Allergy Testing. Penicillin skin testing is reasonably well standardized and, if negative, can exclude the possibility of anaphylaxis to penicillin or other beta-lactams enough to allow treatment. This could be clinically relevant given cited statistics that perhaps only 15% of patients who report an allergy to penicillin are actually skin test positive. • Venom Immunotherapy. For patients who have had anaphylactic reactions to hymenoptera stings, venom immunotherapy will decrease the risk of recurrent anaphylaxis if stung again. Skin testing can help identify which patients should undergo immunotherapy for hymenoptera venom. • Food Allergy Testing. More common in the pediatric population than adults, skin testing to food allergens is less standardized and carries less diagnostic accuracy than testing for inhalant allergens such as grasses, trees, pollens, and molds. • Allergic Contact Dermatitis. Patch testing, in which common inducers of allergic contact dermatitis are applied and the skin subsequently checked for a reaction, is another method of allergy testing.
References • Gendo K, Larson EB. Evidence-based diagnostic strategies for evaluating suspected allergic rhinitis. .Ann Intern Med. 2004 Feb 17;140(4):278-89. • Terreehorst et al, Evaluation of impermeable covers for bedding in patients with allergic rhinitis. N Engl J Med 2003 Jul 17;349(3):237-46