Download
1 / 44
440 likes | 448 Views
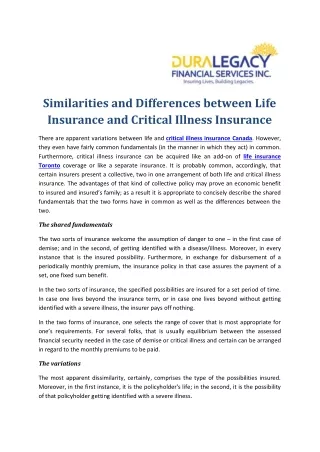
The Association between Late-life Depression and Medical Illness.

E N D
The Association between Late-life Depression and Medical Illness Maria D. Llorente MD Professor Dept. of Psychiatry & Behavioral Sciences Miller School of Medicine at the University of Miami
The “Graying” of America • By the year 2025, the world’s older population (60 and older) will approach 1.2 billion. • By the year 2030, 1 of every 5 people in the U.S. will be 65 or older. • Older Americans will number more than 65 million
Late-Life Depression • Incidence of major depression declines with age, but minor depression is much more common • Depressive symptoms occur in 15%–25% of older adults (>65 years) that fail to meet criteria but cause distress and interfere with functioning • Fewer than half of depressed seniors are recognized as being depressed and of those who are identified fewer than half receive treatment U.S. Dept of Health and Human Services. Mental Health: A Report of the Surgeon General. Rockville, MD: U.S. Dept of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, NIH, NIMH, 1999.
Primary Care is the De Facto Mental Health System (in the United States) responsible for the care of more patients with mental disorders than the specialty mental health sector. Regier et al. Arch Gen Psychiatry 1993; 50:85-94
Epidemiology of Major Depression • 16.2% of US population report at least one lifetime episode • More than half of patients have first episode by age 40 • 25% of older cancer patients • 25-50% of post-stroke patients • 1/3 of Alzheimer’s patients • 50% of Parkinson’s patients • 30% of post-MI Patients Depression Guideline Panel. Depression in Primary Care: Vol 1. Detection and Diagnosis. Clinical Practice Guideline No. 5. Rockville, MD: US Dept of Health and Human Services. Public Health Service, Agency for Health Care Policy and Research; no. 93-0550; 1993. Kessler RC et al. J Affect Disord. 1993;29:85-96. Kessler et al., JAMA 2003; Evans et al., J Clin Psych 1999; Astrom et al., Stroke, 1993; Tiller et al., Psychopharm 1992; Meaf et al., Neurology 1994; Cumming Am J Psych 1992.
HISPANIC >65 will increase by more than 450% by 2050 Depressive disorder prevalence in primary care increased from 4.5% to 8.6% between 1992-97 Higher prevalence of depressive symptoms (11-40%) Higher depression-associated mortality from both suicide and medical disorders AFRICAN-AMERICAN >65 will increase by 131% by 2030 Lower rates of depression recognition and treatment Poorer medical outcomes associated with comorbid depression (EX: diabetes and stroke/hyperglycemia/renal failure/hypertriglyceridemia) Minority Elderlyand Depression
Major Depression Is Associated with Chronic Medical Illness 6%–25% Prevalenceof Major Depression (%) 6%–14% 5%–10% 2%–4% Katon W, Schulberg H. Gen Hosp Psychiatry. 1992;14:237-247. Rosen J, Mulsant BH, Pollock BG. Nursing Home Med. 1997;5:156-165.
Patient morbidity Poorer health outcomes Suicide attempts Accidents Lost jobs Alcohol Use & Abuse Marital Problems Mortality Older white men have highest suicide rates Fatal accidents Death due to related medical complications Societal costs Caregiver burden Higher medical costs Increased healthcare utilization Impact of Untreated Depression: Morbidity & Mortality Preskorn SH. Outpatient Management of Depression: A Guide for the Primary Care Practitioner. 2nd ed. Caddo, OK: Professional Communications, Inc.; 1999: Chapter 2.
100 95 90 85 80 75 70 0 Comparison of Physical and Social Functioning in Other Medical Illnesses Depression impairs physical and social functioning significantly more than these medical illnesses * * * * * Social or Physical Functioning Score† * * * * P <0.05 vs depressive disorder. † Score of 100 = perfect functioning. Wells KB et al. JAMA. 1989;262:914-919.
Major Depression: Post-MI Survival OR = 3.6 % Cardiac Mortality Depressed (N=35) Non-depressed (N=187) 0 6 12 18 months Frasure-Smith, Lesperance, 1998
Major Depression and Congestive Heart Failure • More severe medical illness and more functional impairment than non-depressed (Freedman 2001) • Utilize more inpatient/outpatient medical services than non-depressed (Koenig, 1998)
Major Depression and Congestive Heart Failure • Associated with increased risk of functional decline or death at 6 month f/u (Vaccarino, 2001) • Depression is significant predictor of mortality in clinically stable CHF patients (Murberg, 1999) • Greater severity of depression associated with 3-fold increased risk of mortality at 1 year f/u than non-depressed (Jiang, 2001)
Major Depression and Diabetes Mellitus • 28% of sample reported moderately severe symptoms of depression and/or anxiety • Significant association between depressive symptoms and high Hgb A1C in men • 1/3 reported they’d like counseling Lloyd et.al. Diabet Med 2000 Mar;17(3):198-202
Major Depression and Diabetes Mellitus • Medline and PsycINFO databases and published reference lists were used to identify studies that measured the association of depression with glucose control. • A total of 24 studies satisfied the inclusion and exclusion criteria for the meta-analysis. • Depression was significantly associated with hyperglycemia (Z = 5.4, P < 0.0001). Lustman et.al. Diabetes Care 2000 Jul;23(7):934-42
Major Depression and Diabetes Mellitus • 183 African-American men with diabetes • 30% had significant depressive symptoms (CES-D >22) • Greater depressive symptoms significantly associated with higher serum levels of cholesterol and triglycerides (P<0.050). Gary et.al. Diabetes Care 2000 Jan;23(1):23-9
Medical Illness, Depression and Suicide • Record-linkage of 2323 suicides among 1.9 million people 50 and older in Denmark showed that neoplasms, circulatory/respiratory and digestive diseases confer increased risk; infections, nutritional, metabolic diseases increased risk for hospitalized men; did not control for mood disorders (Erlangsen et al; JAGS 2005) • Pulmonary disease, cancer, visual impairment and neurological disorder confer risk after adjusting for mood disorders (Waern et al; BMJ 2002)
Suicide Rates By Age & Gender (Per 100,000) CDC. National Center for Health Statistics; 2000
Suicide and Lifetime Axis I Diagnosis By Age Conwell, Am J Psychiatry, 1994
Reasons for Underdiagnosis of Late-life Depression in Primary Care • Over-identification with the patient • Lack of time • Lack of training in mental health • False belief that older adults won’t respond to treatment • Atypical symptoms in older adults
Sleep: Insomnia or hypersomnia Interest*:Depressed mood* Loss of interest* Guilt: Feelings of worthlessness Energy: Fatigue Concentration: Diminished ability to think or make decisions Appetite: Weight change Psychomotor: Psychomotor slowing or agitation Suicide: Preoccupation with death DSM-IV-TR Criteria for Major Depression 5 Symptoms in the same 2-week period * Must include 1 of these DSM-IV-TR. Washington, DC: American Psychiatric Association. 2000.
Clinical Features of Late-life Depression • “Depression” without sadness • Irritability • Prominent Anxiety • Cognitive complaints • Prominent vague somatic complaints • Unexplained health worries • Heightened pain complaints • Loss of interest and pleasure • Social withdrawal or avoidance of social interactions • Multiple primary care visits without resolution of the problem • Unexplained functional decline
Early-onset Index episode in childhood or early adult life First degree relatives with depression Less physical illness More psychiatric comorbidity (SUD; personality disorders) Sad mood Late-onset Index episode after age 50 Less genetic predisposition Chronic physical illness Poorer treatment response with more chronic course Increased mortality Abnormal brain imaging Les psych comorbidity Apathy and anhedonia Early-onset v. Late-onset
Phases of Treatment for Depression Remission Relapse Recurrence Euthymia + Relapse Increasedseverity Symptoms Response Progression to disorder + Syndrome Acute (6–12 wk) Continuation (4–9 mo) Maintenance ( 1 yr) Treatment phases Time Kupfer DJ. J Clin Psychiatry. 1991;52(suppl 5):28.
Treatment Goal The goal of treatment with either antidepressant medication or psychotherapy in the acute phase is the remission of major depressive disorder symptoms APA Practice Guidelines for the Treatment of Psychiatric Disorders. 2000.
Pseudodementia • Patients may present with complaints of loss of memory • Frequent “I don’t know responses” on exam • Often a prodrome of dementing illness (as many as 50% may develop dementia within 5 years) • If prodromal, usually late-onset, with prominent psychomotor retardation and/or psychotic features • Consider frequent neurocognitive testing, and early use of cognitive-enhancing agents.
Vascular depression • Frontostriatal disconnection/dysfunction (Executive dysfunction – impairment in IADLs) • Prominent psychomotor slowing and apathy • Poorer response to treatment, higher risk of relapse and recurrence • Limited vegetative symptoms and little depressive ideation • Brain imaging abnormalities: enlarged ventricles, white matter hyperintensities
3-6 months after CVA Prominent vegetative features Larger lesion volumes Likely biological pathogenesis 12-24 months after CVA Fewer vegetative symptoms, more apathy Associated with significant social and physical impairments Post-stroke depression
Depression with Psychosis • 4% of depressed elderly • 45% of psychiatrically hospitalized elderly • Frequent and severe anxiety and agitation • Somatic delusions common, but few hallucinations • Nihilistic beliefs, hopelessness • Often have suicidal ideations • ECT indicated as first-line treatment
Minor Depression • Subsyndromal Depression • Associated with significant functional impairment and disability, lower quality of life and increased medical care utilization • Associated with progression to depression at one year follow-up • DSM-IV-TR: qualitatively similar to major depression, but only 2-4 symptoms needed
Caregiver Depression • Often seen in those caring for older adult with dementia • Associated with changing roles, increased responsibility, risk of social isolation, grief surrounding loss of demented person • Often fail to recognize stress/burden, but report fatigue, insomnia, social withdrawal, and feeling “burned out” • Affects quality of caregiving
Caregiver Depression Barriers to open discussion: • Need to protect themselves from feelings of disloyalty due to “complaining about” loved one • May represent failure as caregiver • Family already burdened with demented loved one, don’t want to add to burden • Fear of own feelings of anger, guilt, ambivalence • Need to approach from the perspective of enhancing the care provided
Family Intervention and Nursing Home Placement Mittelman, JAMA 1996
Bereavement • Losses frequently encountered in late-life that lead to bereavement • Features that distinguish depression from bereavement: • Guilt • Suicidal thoughts • Morbid preoccupation wit h worthlessness • Psychomotor retardation • Prolonged and marked functional impairment • Complex hallucinations (not just thinking they heard voice of loved one, or transiently saw their image
Comorbidity of Depression & Anxiety • Nearly 3/4 of community-dwelling adults with lifetime Major Depression also meet criteria for at least 1 other DSM-IV diagnosis • Most (59.2%) of these are anxiety disorders Kessler et al., JAMA 2003 • 86% of older adults with anxiety disorders also met criteria for a depressive disorder PRISM-E, (Bartels et al, Am J Psych 2005)
Comorbidity of Depression & Anxiety • In older adults, comorbid anxiety disorder and depression is associated with: - greater symptom severity - poorer social functioning - more difficult course of illness - decreased or delayed treatment response - higher level of suicidality Angst 1999, Roy-Byrne 2000, Lenze 2000, 2001, Bartels 2002
A randomized, double-blind, flexible-dose study 24 wk treatment Citalopram (Celexa) N = 52 Paroxetine (Paxil) N = 52 Dose range: 20–40 mg/d Outcome measures: HAMD-24, HAMA Outpatients age18–65 years DSM-IV major depression and mixed anxiety/depression HAMD-24 baseline score 18 for depressive symptoms HAMA baseline score 17 for anxiety symptoms Do Anxiety Symptoms Also Respond to Antidepressant Medication Treatment? Study Design Inclusion Criteria Jefferson J, Greist JH. Poster presented at APA, 2001.
Effects on Depression: Citalopram vs Paroxetine Treatment Week 20–40 mg/d(n = 52) 20–40 mg/d(n = 52) HAMD-24Mean ChangeFrom Baseline Jefferson J, Greist JH. Poster presented at APA, 2001.
Effects on Anxiety: Citalopram vs Paroxetine Treatment Week 20–40 mg/d(n = 52) 20–40 mg/d(n = 52) HAMAMean ChangeFrom Baseline Jefferson J, Greist JH. Poster presented at APA, 2001.
Hypotheses for Low Remission Rates in Major Depression • Patients satisfied with incomplete response • Patients, clinicians do not expect remission • Treatments may not be well tolerated • Physicians not comfortable or familiar with recommended optimal dosages Keller MB, et al. Arch Gen Psychiatry. 1992;49:809-816.
Electro-convulsive therapy Indicated in patients who: • Are acutely suicidal • Have major depression with psychotic features • Have failed 2 adequate trials of antidepressants • Cannot tolerate antidepressant tx • Have previously responded to ECT and prefer this tx Patients on average need 6-8 treatments
General Principles of Late-life Depression Management • Education for patient/family that meds are not effective until patient has taken them for the right amount of time (usually 3-6 weeks) in the right dose • Start low, go slow, but go – need to reach therapeutic dose • Minimum duration is 9-12 months after symptom remission for first episode • Recommend long-term treatment in patients with 2 or more lifetime episodes
Evidence-based Management of Late-life Depression • Annual screening for depression in all patients • Patients who screen positive are assessed within 6 weeks for a depressive disorder and/or suicidal ideas • Those who assess positive require treatment with either therapy/ medication alone or in combination • At least 3 follow-up visits within first 3 months • Index episode treated for at least 9-12 months • Recurrent episode maintained on antidepressant long-term