Download
1 / 135
1.58k likes | 2.66k Views
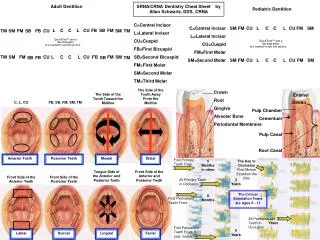
Pulp Therapy in the Primary dentition. Anatomical Features in primary teeth. Dentin: Wide dentinal tubuls ; Additional channels over the pulp horns; Wide dentinal canals above the root delta; Pulp: Maturity level of pulp; Size of the pulp chamber ; Width of the root canals.

E N D
Anatomical Features in primary teeth • Dentin: • Wide dentinal tubuls; • Additional channels over the pulp horns; • Wide dentinal canals above the root delta; • Pulp: • Maturity level of pulp; • Size of the pulp chamber ; • Width of the root canals.
physiologycalfeacures in the primary teeth • Degree of development of root canals: • Formation of root walls; • Formation of the apex; • physiological resorption: • Degree of root degradation; • Reactivity of the pulp; • Degree of development of the alveolar bone.
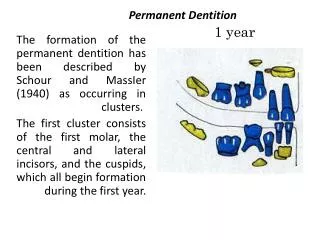
Priod of development of primary molars 4 yrs. 5 yrs pre eruptive period Root construction Functional period Root resorption
Infected and inflamated dental pulp • There are several reasons for a dental pulp to become inflamed, but the far the commonest is as a sequel to dental caries; • Dental caries in primary tooth progresses rapidly to relatively thin enamel and penetrates dentin; • The insult from bacterial toxins stimulates the underlying pulp to respond by mounting an inflammatory reaction – reversible pulpitis.
Etiology of pulp inflamation • Infection: • For deep cavities; • Secondary caries; • It is caused by: • microorganisms; • Microbial toxins; • Dentinal degradation products.
Pathogenetic mechanisms of pulp inflammation Microorganisms Exo-and endotoxins Degradation of odontoblastic processes They are moving through dentine tubules They are reaching to odontoblasts and nerve receptors
From the nerve receptors Is induced reflective Overcoming reaction protection Protection When compensatory mechanisms are running out Inflammation
inflammation • Exudation; • Alteration; • Proliferation.
If a microbes invade the pulp tissue • Causing a massive increase in pulpal response; • This is characterised by irreversible inflmmation and tissue necrosis directly adjacent to the site of exposure; • Bacteria and their products will progress through the pulp tissue, resulting in irreversible inflammation; • The response of pulpal and periodontal tissues to such injury can lead to one of several outcomes:
The periradicular tissues may affected (periradicularperiodontitis), with eventualy involvement of associated tissue; • If the exposure site involves a large area, Hyperplasticpulpitis (pulp polyp) may occur; • The tooth may be subject to pathological resorption – for example, internal inflammatory resorption.
Used until now classification resulting from the old concept • Acute pulp inflammation: • Pulpitisacutaserosapartialis; • Pulpitisacutaserosatotalis; • Pulpitisacutapurulentapartialis; • Pulpitispurulentatotalis; • Chronic pulp inflammation: • Pulpitis chronicаfibrosa; • Pulpitis chronicаulcerosa; • Pulpitis chronic а granulomatosa.
In exacerbation of chronic pulpitis of a primary teeth processes are passing very quickly from one phase to another.
Irreversible pulpitis Contemporary classification of pulpitis Reversible pulpitis
Types of stem cells morula
Proof of stem cells from the pulp of the primary teeth The red coloration indicates the presence of nestin; Green staining demonstrated the presence of actin
Pulp Therapy in the Primary teeth The treatment plan should be based on specific diagnosed findings, medical status and the child's behavior, social status of the family.
The most common pulpitis of primary teeth • Reversible - closed asymptomatic pulpitis; • Large carious lesions without pulp symptom "pain"; • Pulp symptom "pain" is: • Spontaneous pain; • Night pain; • Provoked pain - over 1 min; • Occurrence of pain while eating or irritation in carious lesions still does not mean pulp symptom "pain".
Criteria for diagnosis "Reversible pulpitis of the primary teeth"
clinical findings Large cavitated carious lesions with: 1.Soften lighter or darker carious dentin; 2. Lack of disclosure of the pulp (pulpitis closed); 3. Cavitation affects closest cusp; 4. The reserved portion is less than ½ of the distance between the tip of the cusp and fissure.
Small cavitation, but staining near the cusps, especially at medio-vestibular pulpal horns of the first primary molars
Approximal carious lesions covering the entire interproximal wall