Download
1 / 28
350 likes | 1.1k Views
Lungs and Alveoli. You must be able to draw the structure of the lungs and alveoli. http://www.people.eku.edu/ritchisong/301notes6.htm. Lung Anatomy. http://sprojects.mmi.mcgill.ca/resp/anatomy.swf. Why and how do we breathe?. http://www.airinfonow.org/html/lungattack/lungplay.htm.

E N D
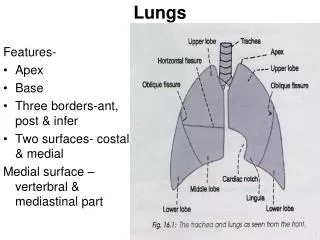
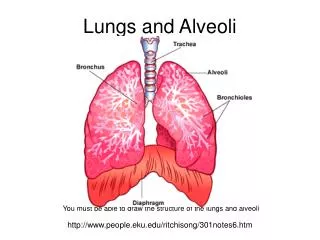
Lungs and Alveoli You must be able to draw the structure of the lungs and alveoli http://www.people.eku.edu/ritchisong/301notes6.htm
Lung Anatomy http://sprojects.mmi.mcgill.ca/resp/anatomy.swf
Why and how do we breathe? http://www.airinfonow.org/html/lungattack/lungplay.htm
The need to ventilate • A ventilation system is needed to maintain concentration gradients in the alveoli • The steep concentration gradient across the respiratory surface is maintained in two ways: by blood flow on one side and by air flow on the other side. The ventilation system replaces diffuses oxygen (keeping the concentration high) and removes carbon dioxide (keeping the concentration low). • This means oxygen can always diffuse down its concentration gradient from the air to the blood, while at the same time carbon dioxide can diffuse down its concentration gradient from the blood to the air.
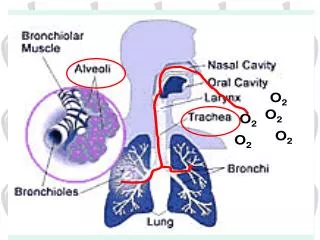
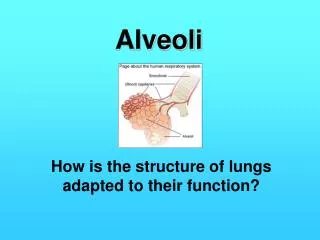
Features of the alveoli • large surface area: surface area of the alveolar epithelium - 100 m2 • thin: single cell layer of epithelium across which diffusion occurs • moist: gasses need to dissolve before passing membranes • rich blood supply: extensive net of capillaries for transport of gasses to and from alveoli
Intercostal muscles contract. Ribs move out and ______ Diaphragm contracts and gets ____________ Inhalation Volume _____________ Pressure ____________ Air enters the lungs
The lungs relax here and the pressure inside and outside the lungs goes back to normal atmospheric pressure 760mm Hg
Intercostal muscles ______. Ribs move ___ and ______ Diaphragm _______ and returns to its dome shape Exhalation Volume _____________ Pressure ____________ Air _____ the lungs
Lowering of the diaphragm and rising of the ribs causes a drop in air pressure of 4mm Hg
Gas exchhange • Howstuffworks "Gas Exchange"
HL: Partial pressure • In summary, gases move from a region of higher partial pressure to a region of lower partial pressure. • Animations partial pressure. Keep in mind above summary.
Partial Pressures of O2 and CO2 in the body (resting) • Alveoli • PO2 = 100 mm Hg • PCO2 = 40 mm Hg • Alveolar capillaries • Entering the alveolar capillaries • PO2 = 40 mm Hg (relatively low because this blood has just returned from the systemic circulation & has lost much of its oxygen) • PCO2 = 45 mm Hg (relatively high because the blood returning from the systemic circulation has picked up carbon dioxide)
How are oxygen & carbon dioxide transported in the blood? • Oxygen is carried in blood: 1. bound to hemoglobin (98.5% of all oxygen in the blood) 2. dissolved in the plasma (1.5%) • Animation Quizzes hemoglobin
The graph below shows the Haemoglobin- Oxygen Association Curve. This shows the % of oxygen in the blood (oxyhaemoglobin) and the partial pressure of O2 in the environment.Simply put it means that oxygen joins haemoglobin and stays joined at high partial pressures of oxygen. When the level of oxygen is low (low partial pressure), the oxygen molecules dissociate (jump off) the haemoglobin molecule. The more O2 a molecule of Hb accepts, the easier it is to carry more, as it changes its shape.
Mammalian muscles also contain a chemical called Myoglobin. It is similar, but smaller than haemoglobin. It holds onto oxygen much more tightly (higher affinity) and only dissociates at much lower partial pressures- a store of oxygen for difficult times.
In the developing foetus, the haemoglobin has a much higher affinity for oxygen. This means that the baby can absorb oxygen efficiently across the placenta at fairly low partial pressures.
The Bohr Shift: When there is lots of CO2 due to respiration, the acidity of the blood increases slightly. This causes the whole graph to shift to the right (and get steeper). This allows oxygen to unload at these places even easier.
High altitudes People who live at high altitude have to cope with having less O2 available for respiration. Their body compensates by making far more haemoglobin. This increases the amount of oxygen that can be carried. However, there is a downside: when there is too much haemoglobin, blood becomes sticky and viscous and it is harder for the heart to pump the blood around the body. This happens in chronic mountain sickness. Athletes often train at altitude- this can benefit them when they return to run races, as they have an improved exchange rate with more haemoglobin
CO2 produced in mitochondria • Diffuses out into tissues and tissue fluid • In rbc it combines with H20 forming carbonic acid • (H2CO3) using carbonic anhydrase. • This splits (dissociates) into H ions and HCO3 ions • Haemoglobin acts as a buffer and takes the H ions to form Haemoglobonic acid (H.Hb) • The blood stays fairly neutral and can absorb lots of CO2 • As the amount of HCO3 rises in the rbc, they start to diffuse out down the conc. gradient into the plasma • This cannot be balanced, as the cell stops ions like Na and K • The cells would get more and more positively charged (compared to the plasma) and prevent O2 uptake • Chloride ions are pumped in from plasma to balance it- called the chloride shift • At the lungs the oxygen is taken up by dissolved H.Hb- forming Hb.O2 • H ions are released and combine with HCO3 forming carbonic acid- the CO2 then diffuses out • The HCO3 content falls, so more moves in from the plasma, so more CO2 released • The chloride shift moves ions into the plasma to maintain neutrality
What is asthma? In asthma, the muscles lining the airways are very sensitive and overreact to substances or events, known as triggers, that other people tolerate without problem. Often pollen, dust, mould spores and smoke can cause this, but often other allergens can trigger it too. 3 things generally happen: • Tightening of the muscles lining the airways • Mucus production • Inflammation Imagine having done 3 minutes exercise, then try to recover, but ONLY breathing through a straw!! http://video.about.com/asthma/Asthma.htm http://kidshealth.org/misc/movie/cc/how-asthma-affects.html
Lung volumes • Tidal volume – the amount of air breathed in or out of the lungs in a normal breath. This is about 500cm3 • Inspiratory reserve volume – extra lung volume available if you breathe in as much as you can. This is about 3000cm3 • Expiratory reserve volume – extra lung volume available if you breathe out as much as you can. This is about 1100cm3
Lung volumes • Vital capacity – this is the TV + IRV + ERV or the useable lung capacity. It is about 4500cm3 • Residual air – this is the amount of air that needs to stay in your lungs to stop them collapsing. It is about 1200cm3
Lung capacity practical • Look at the instructions for how to use the lung volume kit. • Try to measure your own lung volume • Plan an investigation into a factor that could affect vital capacity.