Download
1 / 48
480 likes | 743 Views
Alyssa Morris, R4 September 30, 2010. Mx of UA and NSTEMI. OBJECTIVES. Mx of UA/NSTEMI in the ED CRUSADE, COMMIT, ISIS-2, CAPRIE, CURE, PCI-CURE, OASIS-5, OASIS- 7, SYNERGY NOT covering GPIIb/IIIa inhibitors Statins Decision to go to PCI or medical management Variants of ACS.

E N D
Alyssa Morris, R4 September 30, 2010 Mx of UA and NSTEMI
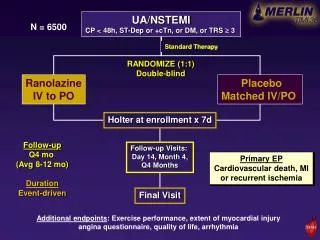
OBJECTIVES • Mx of UA/NSTEMI in the ED • CRUSADE, COMMIT, ISIS-2, CAPRIE, CURE, PCI-CURE, OASIS-5, OASIS- 7, SYNERGY • NOT covering • GPIIb/IIIa inhibitors • Statins • Decision to go to PCI or medical management • Variants of ACS
LEVEL OF EVIDENCE • See handout
TERMINOLOGY • Stable Angina • Angina brought on by exertion and relieved with predictable measures (rest/NTG) • Unstable Angina/ACS • New onset angina w/i 2/12 and at least CCS III • Rest angina lasting >20min w/i 1wk of angina • Change from baseline • NSTEMI/ACS • + markers
TERMINOLOGY • Acute Coronary Syndromes is the preferred terminology to refer a spectrum of disease related to myocardial ischemia (stable angina) Unstable Angina NSTEMI STEMI +/- abN ECG, -ve markers +/- abN ECG, +ve markers STE on ECG, +ve markers
CASE • 60M with RSCP with a +TNT at 6 hrs after pain started, no STE on multiple ECGs • BP= 176/98, P= 90, 02= 94% • How would you treat this person? • Write down all that you would do • What do you think the NNT for each of your therapies is?
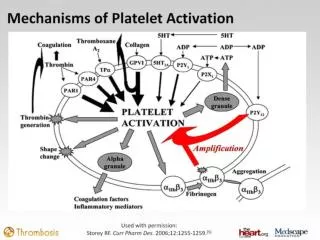
TREATMENT STRATEGIES • ANTI-ISCHEMIC • Inc supply: nitrates, oxygen • Dec demand: BB, morphine, ACE-I • ANTI-PLATELET • ASA, Clopidogrel, GPIIb/IIIa inhibitors • ANTI-THROMBOTIC • Medical: UFH, LMWH, thrombolytics • Invasive: PCI/CABG • ANTI-INFLAMMATORY • Statins
OXYGEN- AHA guidelines LOE: B • Administered to UA/NSTEMI pts with: • Sa02<90% • Respiratory distress • Other high-risk features for hypoxemia LOE: C • Reasonable to administer to all patients in 1st 6hrs from presentation
NITRATES • Reduces myocardial oxygen demand while enhancing myocardial oxygen delivery • Venous dilation • Arterial dilation • Peripheral and coronary arteries
NITRATES- AHA guidelines LOE: C • Sublingual NTG for ongoing ischemic discomfort • 0.4mg Q5min, max of 3 doses • Assess need for IV NTG • Persistent pain, HF, HTN • Q: How do you titrate your nitro drip? • Not if SBP<90, HR<50, PDE I in last 24-48hr
MORPHINE- AHA guidelines • Venodilation • Modest reductions in HR (inc vagal tone) • Modest reductions in SBP CLASS IIa/ LOE B • Reasonable to administer it IV if uncontrolled ischemic chest pain despite NTG • Provided you use additional therapy to manage the ischemia
Nonrandomized, retrospective, observational study • N= 57,039 (w NSTEMI) • 17,003 (29.8%) received morphine • Higher adjusted risk of death (OR 1.48, 95% CI 1.33-1.64
BETA BLOCKERS • Competitively block the effects of catecholamines on cell membrane R • Reduce myocardial contractility • Reduce sinus node rate • Reduces AV node conduction velocity
Randomized trial • N= 45,852 • 93% had STE or LBBB • 7% had NSTEMI • Randomized to metoprolol or placebo • IV max 15mg then 200mg PO OD • No reduction in composite of death, reinfarction or cardiac arrest • Less VFIB later in study • Increased risk of cardiogenic shock in 1st day
BETA BLOCKERS- AHA guidelines • CLASS I/ LOE B • Oral BB should be started w/i 24hr in patients who do not have 1 of: 1) Signs of HF, 2) low-output state, 3) increased risk for cardiogenic shock, 4) other contraindications to BB • CLASS II/ LOE B • Reasonable to administer IV BB at timeof presentation for HTN who do not have 1 of above
CCBs • Reduce cell transmembrane inward Ca flux • Inhibits myocardial and vascular smooth muscle contraction • Some also slow AV conduction and depress sinus node impulse formation • Verapamil and diltiazem • Coronary dilation • Benefit is from reduced myocardial oxygen demand and improved myocardial flow
CCBs- AHA guidelines • CLASS I/ LOE B • NondihydropyridineCCBs should be given to pts with ongoing or frequently occurring ischemic pain in whom BB are contraindicated • Not if LV dysfunction or other CIs • CLASS IIb/ LOE B • Can use ER nondihydropyridine CCB instead of a BB • Can only use IR dihydropyridine in adequately BB pt
ACE-I – AHA guidelines • CLASS I/ LOE A • Should be started orally w/i 24h in pts with pulmonary congestion or LVEF <0.4 in absence of hypotension (SBP<100) • CLASS IIa/ LOE B • Can be used in patients w/o pulmonary congestion or LVEF <0.4 • CLASS III • IV should not be given in the 1st 24h b/c of increased risk of hypotension
NSAIDS- AHA guidelines • CLASS I/LOE C • b/c of increased risk of mortality, reinfarction, htn, HF and myocardial rupture associated with their use, NSAIDs (except ASA) should be discontinued and not administered
ASA • Irreversibly inhibits COX-1 w/i platelets • Diminishes platelet aggregation • Fully present even with low dose
Meta-analyses of RCTs • 195 trials, 143,000 patients • 22% reduction in the odds of vascular death, MI, or stroke • ARR 6.1%, NNT 16 • 75mg to 1500mg of ASA showed similar reductions in the odds of vascular events
RCT • N= 17,187 pts with suspected acute MI • Randomized to 1month of ASA • 26 fewer deaths per 1000 during first 35d • ARR for 35d mortality 2.4% • RRR for 35d mortality 23% • NNT=43 (to prevent one death) • Showed benefit if given early
ASA- AHA guidelines • CLASS I/ LOE A • ASA should be administered asap and continued indefinitely • In pts with hx of GIB a PPI should be used • CIs • Intolerance and allergy • Active bleeding • Hemophilia • Severe untreated htn
PLAVIX • Platelet effects are irreversible but take several days to achieve • Loading dose shortens this time substantially • Different mechanism than ASA • Potential exists for for additive benefit • Adenosine diphosphate receptor antagonist
Randomised, blinded international study • Efficacy of ASA and Clopidogrel (75mg OD) in reducing risk of a composite of ischemic stroke, MI, vascular death • N= 19,185, Included recent ischemic stroke, MI or symptomatic peripheral artery dz • Plavix annual risk of 5.32% vs ASA 5.83% (P=0.043) (NNT= 194) • No difference in AE
RCT • N= 12,562 with UA/NSTEMI • Placebo or Clopidogrel (300mg loading dose then 75mg daily) • All pts received ASA • Outcome: 1) composite of death from CV cause, MI or stroke 2) refractory ischemia • Results: 1) placebo 11.4% vsClopidogrel 9.3% 2) placebo 18.8% vsclopidogrel 16.5% (p<0.001) (20% RRR, 2.1% ARR, NNT= 48)
Observational substudy of CURE • N= 2658 pts undergoing PCI • Received the loading dose of Plavix then daily for 10 days, then they got thienopyridine for 4 weeks, then plavix restarted • Outcome: composite of death, MI or urgent revascularization • Results: placebo 6.4% vsclopidogrel 4.5% (p=0.03) (ARR= 3.8%, NNT= 26)
RCT • 45852 pts, 7% had UA/NSTEMI • Plavix 75mg OD or placebo • Outcomes: 1) composite of death, reinfarction or stroke; 2) death from any cause • ARR 0.9% and NNT 111 • Concluded that adding plavix to ASA safely reduces mortality and major vascular evens and should be done routinely
Plavix- How much? • Approved loading dose in UA/NSTEMI is 300mg • 600mg does achieve antiplateletfxn more quickly • Not enough good evidence to use this much • Considerable inter-individual variation in antiplatelet effect with all loading doses • O mg if you believe pt going to CABG • Increased risk of minor bleeding • Some believe benefit outweighs risk
RCT2x2 factorial design • N= 25,086 w ACS, >70% had UA/NSTEMI • Invasive strategy + loading dose of 600mg Plavix or 300mg Plavix • High or low dose ASA also given randomly • Outcome: cardiovascular death, myocardial infarction or stroke at 30d • 4.2% in high Plavixvs 4.4% standard Plavix • Secondary outcome of stent thrombosis in those with PCI (HD 1.6% v SD 2.3%, p= 0.001)
PLAVIX – AHA guidelines • CLASS I • Plavix should be given to pts who are unable to take ASA (LOE A) • Pts with hx GIB should get a PPI if getting Plavix (LOE B) • Plavix should be given to pts in addition to ASA in pts who are receiving an initial invasive stratgey (LOE B) • Plavix should be given to pts in addition to ASA in pts who are receiving conservative therapy (LOE B)
UFH • UFH • Accelerates action of antithrombin inactivates factor IIa (thrombin), factor IXa and Xa • Prevents thrombus propagation but does not lyse existing thrombi • Binds to a number of plasma proteins, blood cells and endothelial cells
LMWH • LMWH • From depolymerization of chains of heparin • Inactivate Xa>IIa(b/c of molecular weight) • Advantages: • decreased binding to plasma proteins and endothelial cells • Dose-independent clearance • Longer half-life that results in more predictable and sustained anticoagulation w SC administration
Synthetic Factor Xa Inhibitors • Fondaparinux • Synthetic pentasaccharide • Acts proximally in cascade to inhibit multiplier effects of the downstream coagulation rxns reduce amount of thrombi that is generated • Indirect, selective factor Xa inhibitor • Binds to antithrombin III • Same advantages as LMWH
Prospective, randomized, open-label • N= 10027 high-risk UA/NSTEMI pts w early invasive strategy • Compare enoxaparin to UFH for composite endpoint of all-cause death or MI in 30d • 14% in enox group vs 14.5% in UFH group (p=0.4) • More bleeding in enox group • Post-hoc showed from switching type of anticoagulant at time of PCI
Low molecular weight heparins vsunfrctionated heparin for acute coronary syndromesMagee KD, Sevcik W, Moher D, Rowe BH • To assess the effects of LMWH compared to UFH for ACS (UA/NSTEMI) • 7 studies involving over 10,000 people • No difference in overall mortality • LMWH showed reduced recurrence of MI and the need for revascularization procedures • No difference in recurrent angina, major bleeds, or minor bleeds; there was a decrease in the incidence of HIT • 125 patients have to be treated with LMWH to prevent 1 MI, and 50 have to be treated to prevent 1 revascularization procedure Cochrane Database of Systematic Reviews 2003
N= • RCDBT, industry sponsored, non-inferiority • N= 20,078, UA/NSTEMI patients • Enox 1mg SC BID v Fonda 2.5mg SC OD • + UFH at PCI if last dose >6hr ago • Outcomes: 1) death, MI or refractory ischemia at 9d; 2) major bleeding • 1) 5.8% wfondav 5.7% wenox • Satisfies non-inferiority criteria • 2) 2.2% wfondav 4.1% wenox (p<0.001)
ANTICOAGULANT Mx- AHA guidelines • CLASS I • Should be added to antiplt therapy at presentation • Invasive Strategy LOE A • UFH or Enoxaparin • Invasive Strategy LOE B • Fondaparinux • Conservative strategy LOE A • UFH or enoxaparin • Conservative strategy LOE B • Fondaparinux • Use fondaparinux if increased risk of bleeding
SUMMARY • BB • ASA • NNT 16 in meta-analysis • NNT 43 in ISIS-2 • Plavix • NNT 48 in CURE • NNT 194 in CAPRIE • NNT 26 in PCI-CURE • NNT 111 in COMMIT • Anticoagulant