
Epstein-Barr virus
Epstein-Barr virus. Shane C. McAllister, MD, PhD Pediatric Infectious Diseases Fellow Stony Brook Long Island Children’s Hospital. Overview. History of EBV and mononucleosis EBV structure and gene expression Pathogenesis/Clinical manifestations Epidemiology Diagnosis

Epstein-Barr virus
E N D
Presentation Transcript
Epstein-Barr virus Shane C. McAllister, MD, PhD Pediatric Infectious Diseases Fellow Stony Brook Long Island Children’s Hospital
Overview History of EBV and mononucleosis EBV structure and gene expression Pathogenesis/Clinical manifestations Epidemiology Diagnosis Treatment Cases
INTRODUCTION • Infectious mononucleosis (IM) was first recognized in1920 however the etiology was unknown • The heterophile test was discovered to be diagnostic for Infectious Mononucleosis in 1932 • A viral cause of mononucleosis was suspected in the 1960s when a laboratory worker became ill while working with Burkitt lymphoma tissue samples
INTRODUCTION • In 1968, Epstein-Barr Virus was actually identified as the cause of Infectious Mononucleosis • Since the initial discovery, EBV has been implicated in a wide variety of both benign and malignant diseases
Herpesviruses • 8 herpesviruses known to infect humans • Strict species specificity • Closely related rodent and non-human primate strains used as animal models
Herpesviruses • Large double-stranded DNA Viruses • ≥ 84 different proteins • Maintenance/replication of genome in host cell nucleus
Herpesviruses • Life-long latency with periodiclytic reactivation • Control of infection requires cellular and humoral immunity
Kinetic Classes of EBV Genes • Latency • LMP-1, EBNAs • Immediate Early: initiate lytic cycle • Zta, Rta • Early: condition the host cell environment and synthesize viral DNA • EA-D • Late: structural components of capsids/mature virions • gp350
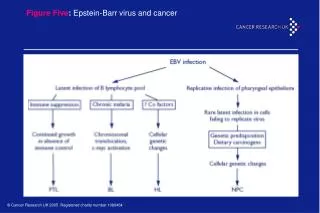
DISEASE ASSOCIATIONS • Infectious Mononucleosis • Chronic Infectious Mononucleosis • Burkitt Lymphoma • Nasopharyngeal carcinoma • Hodgkin Lymphoma • Lymphoproliferative disease • X-linked Lymphoproliferative disease • Oral Leukoplakia (AIDS)
PATHOGENESIS • EBV infection is considered immunopathologic rather than tissue destructive • EBV initially infects and replicates in the oropharyngeal epithelial cells • B-cells are subsequently infected • Infected B-cells disseminate throughout the lymphoreticular system
PATHOGENESIS • EBV infection triggers an impressive but self-limited immune response • Infected B-cells are transformed and secrete a diverse group of antibodies • Heterophile antibodies • Antibodies to specific EBV antigens • Various auto-antibodies • EBV induced polyclonal activation of B-cells also leads to an increase in serum immunoglobulins
PATHOGENESIS • Infected B-Lymphocytes induce T-Lymphocyte proliferation • Manifested as Atypical Lymphocytosis • Proliferation of reactive T-cells and infected B-cells leads to • Lymphadenopathy • Hepatosplenomegaly
CLINICAL MANIFESTATIONS SYMPTOM % RANGE (%) SORE THROAT 82 70 - 88 MALAISE 57 43 - 76 HEADACHE 51 37 - 55 ANOREXIA 21 10 - 27 MYALGIAS 20 12 - 22 CHILLS 16 9 - 18 NAUSEA 12 2 - 17 ABDOMINAL DISCOMFORT 9 2 - 14 COUGH 5 5 VOMITING 5 5 ARTHRALGIAS 2 2
CLINICAL MANIFESTATIONS SIGNS % RANGE (%) LYMPHADENOPATHY 94 93 - 100 PHARYNGITIS 84 69 - 91 FEVER 76 63 - 100 SPLENOMEGALY 52 50 - 63 HEPATOMEGALY 12 6 - 14 PALATAL ENANTHEM 11 5 - 13 JAUNDICE 9 4 - 10 RASH 10 0 - 15
PHYSICAL FINDINGS EXUDATIVE PHARYNGITIS
PHYSICAL FINDINGS TONSILLAR HYPERTROPHY
EBV – Physical Findings • Rash and Antibiotics • Nonspecific maculopapular eruption associated with administration of Ampicillin/Amoxil (50 – 100%) • May be associated with other -lactam antibiotics (40 – 60%) • Usually develops 7 – 10 days after the first dose • Does not represent Penicillin allergy • Mechanism is unclear • Transient hypersensitivity reaction • Immune complex production
Complications of Primary EBV ORGAN/SYSTEMCOMPLICATIONS LIVER: Abnormal Liver Function Tests (80 – 90%) Clinical jaundice (5%) Fulminant hepatitis (rare) RESPIRATORY: Airway Obstruction (<5%) Interstitial Pneumonitis (Rare) HEMATOLOGIC: Thrombocytopenia (25-50% Mild/Mod) Neutropenia (50 – 80% - Mild/Mod) Pancytopenia (Rare) Hemolytic Anemia (3%) Aplastic Anemia (Rare)
Complications of Primary EBV ORGAN/SYSTEMCOMPLICATIONS SPLEEN: Splenic rupture (0.1 – 0.5%) Splenic Infarction RENAL: Hematuria Interstitial nephritis Glomerulonephritis CARDIAC: Myocarditis Pericarditis Arrhythmias
Complications of Primary EBV ORGAN/SYSTEMCOMPLICATIONS SECONDARY INFECTION: Streptococcal pharyngitis Secondary sepsis due to neutropenia IMMUNOLOGIC: Depressed T-cell immunity NEUROLOGIC: Encephalitis Aseptic Meningitis Guillain-Barre Syndrome Cranial nerve palsies Transverse Myelitis Optic Neuritis Cerebellar Ataxia Brachial Plexus Neuropathy
Neurologic Complications • May be the first or sole manifestation of EBV mononucleosis • Occurs in 1 – 5% of cases • Prognosis is generally good with 85% complete recovery • Most frequent cause of death related to EBV Infectious Mononucleosis • Diagnosis is difficult • Heterophile is negative • Atypical lymphocytosis is minimal or absent
Neurologic Complications “Because EBV may present atypically and has been associated with a myriad of neurologic diseases, EBV should be considered in all acute neurologic illnesses of unknown etiology in the Pediatric population” Connelly et al., Pediatr Neurol 1994; 10: 181-184
INFECTIOUS MONO IN CHILDREN • Compared with adolescents, young children more commonly had the following features: • URI symptoms • Rash • Splenomegaly and/or Hepatomegaly • Higher peak leukocyte counts with fewer Atypical Lymphocytes • More frequent neutropenia
EPIDEMIOLOGY • Antibodies to EBV found in all populations • Lower socioeconomic groups- higher prevalence • By adulthood, 90 - 95% of most populations have demonstrable antibodies • In the US, EBV seroconversion occurs before age 5 years in 50% of the population • Second wave in the second decade of life • No predilection for male or female
EPIDEMIOLOGY • In the US - 45.2 cases/100,000/year • The incidence is highest in the 15 - 24 year-old age group • College and military populations have the highest morbidity • Not a reportable disease • No clear seasonal pattern
Epstein-Barr virus Cytomegalovirus Toxoplasma gondii Adenovirus Human herpesvirus 6/7 Hepatitis A Influenza A and B Rubella virus Diphtheria HIV Malignancies DIFFERENTIAL DIAGNOSIS OF MONO-LIKE SYNDROME
DIFFERENTIAL DIAGNOSIS OF MONO-LIKE SYNDROME • CMV mononucleosis is most frequently confused with EBV: • Patients are generally older (Adults) • Pharyngitis and lymphadenopathy – less common • Fever and malaise are the major manifestations • Heterophile negative
Atypical Lymphocytes • Activated T cells responding to the EBV-infected B-cells • Features of Atypical Lymphs: • Larger than mature Lymphocytes • Have vacuolated basophilic cytoplasm
DIAGNOSIS ATYPICAL LYMPHOCYTES
Heterophile Antibody Test • Heterophile antibodies comprise a broad class of antibody characterized by ability to agglutinate antigens on RBCs from different mammalian species • IM heterophile Ab (IgM) does not react with EBV- specific antigens characterized by its ability to react with beef, sheep and horse RBCs • The antigen that stimulates this heterophile ab is unknown
Heterophile Antibody Test • Replaced by the monospot slide test (Antigen-coated beads on a slide) • 15% of patients with IM may be initially heterophile negative and become positive within 2 – 3 weeks • High false negative rate in children less than 4 years (>50%) • False positive rate - 7% • Remains positive for up to 9 months • Sensitivity and specificity: 85%/97%
MONOSPOT NEGATIVE POSITIVE
FALSE – POSITIVE MONOSPOT • Collagen Vascular diseases • Leukemia/Lymphoma • Malaria • Pancreatic Carcinoma • Viral Hepatitis • Other
EBV SEROLOGY • The appearance of antibodies induced by EBV specific antigens correlates with the phase of replication • IgM antibody to VCA appears at the onset of symptoms and typically disappears within 1 – 3 months • IgG antibody to VCA begins to rise shortly after the onset of symptoms • Peaks at 2 – 3 months • Gradually decreases to a steady-state and persists for life
EBV SEROLOGY • Antibodies to EA are not always detectable • IgG to EA begins to rise at the onset of symptoms • Peak concentration occurs at 3 – 4 weeks • Subsequently decreases and disappears • Antibodies to EBNA appear during the convalescent period and persist for life along with anti-VCA IgG • Past infection: • No anti-VCA IgM (Potential for false-positives) • No anti-EA IgG
Interpretation of EBV Serology INFECTION ANTI-VCA-IgMANTI-VCA-IgG ANTI-EA ANTI-EBNA NONE NEGATIVE NEGATIVE NEGATIVE NEGATIVE ACUTE POSITIVE POSITIVE POS/NEG NEGATIVE RECENT POS/NEG POSITIVE POS/NEG POS/NEG PAST NEGATIVEPOSITIVE NEGATIVE POSITIVE
EBV SEROLOGY • Effective lab diagnosis can be made on single acute phase serum sample • Antibody response appears rapidly (onset of symptoms) • Acute and Convalescent phase serum will not demonstrate a significant change in antibody titer
EBV SEROLOGY • Literature supports the general concern that there is considerable variation in the performance of serological test kits for EBV and other infectious agents • VCA-IgM • Cross-reactivity occurs • Especially with other herpesviruses (CMV)
EBV - DIAGNOSIS • The ability of EBV to maintain lifelong latency with low levels of replication and viral shedding results in enduring antigen exposure and continued humoral immune response • Variation of EBV antibody titers may be due to reactivation of latent virus due to infection with another virus and development of cross-reactive antibodies
EBV - DIAGNOSIS • Important to be aware of nuances of serologic testing as well as viral detection for latent viruses such as EBV • Must be cautious with utilization of serologic testing/DNA detection as the sole means for establishing causal relationship between illness and EBV infection
TREATMENT • Supportive care • Avoid contact sports • Corticosteroids for selective complications • Airway obstruction • Massive splenomegaly • Myocarditis • Hemolytic Anemia/ITP • Acyclovir – No clearly documented benefit
ANTIVIRAL TREATMENT • 5 randomized clinical trials conducted to evaluate treatment of Infectious Mononucleosis with Acyclovir (339 patients) • Studies showed no statistically significant benefit or clinical effectiveness • Met-analysis also showed no significance • No evidence that therapy shortens duration of symptoms or prevents complications
![Epstein Barr Virus [EBV] - Named after Epstein and Barr](https://cdn5.slideserve.com/9727845/epstein-barr-virus-ebv-named-after-epstein-dt.jpg)