Hyperparathyroidism
Hyperparathyroidism. Dr Malith Kumarasinghe MBBS (Colombo). Ivar Sandstrom. Swedish Medical Student Discovered Parathyroid gland In 1880 Last major organ Identified in humans. Parathyroid glands - Anatomy

Hyperparathyroidism
E N D
Presentation Transcript
Hyperparathyroidism Dr Malith Kumarasinghe MBBS (Colombo)
Ivar Sandstrom • Swedish Medical Student • Discovered Parathyroid gland In 1880 • Last major organ Identified in humans
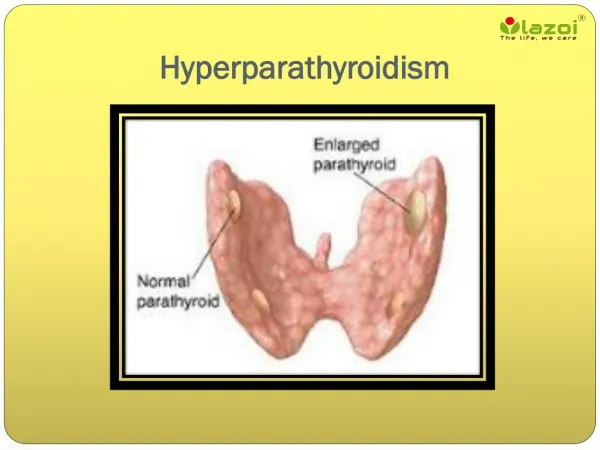
Parathyroid glands- Anatomy • 1. Usually four – two on each side (2-8 is normal) • 2. Lie on the posterior surface of thyroid • 3. May be embedded within thyroid gland • 4. Required for life
Parathyroid Glands (Post. view of thyroid) Parathyroid Glands are located on the posterior aspect of the thyroid; sometimes the tissue is embedded within thyroid tissue.
Low circulating serum calcium concentrations stimulate the parathyroid glands to secrete PTH, which mobilizes calcium from bones by osteoclastic stimulation. PTH also stimulates the kidneys to reabsorb calcium and to convert 25-hydroxyvitamin D3 (produced in the liver) to the active form 1,25-dihydroxyvitamin D3, which stimulates GI calcium absorption. High serum calcium concentrations have a negative feedback effect on PTH secretion. • kk
PTH • Renal effects (steady state maintenance) • Inhibition of phosphate transport • Increased reabsorption of calcium • Stimulation of 25(OH)D-1alpha-hydroxylase • Bone effects (immediate control of blood Ca) • Causes calcium bone release within minutes • Chronic elevation increases bone remodeling and increased osteoclast-mediated bone resorption • However, PTH administered intermittently has been shown to increase bone formation and this is a potential new therapy for osteoporosis
Hypercalcemia - DDX • Parathyroid related • Primary Hyperpara, Li tx, Familial HypocalcuricHypercalcemia • Malignancy • Solid tumor, Hematologic • Excessive Vitamin D • Intoxication, GranulomatousDisease • High bone turnover • Hyperthyroid, Immobilization, VitA • Renal Failure • 2ndary Hyperpara, Aluminum, Milk-Alkali
**Primary hyperparathyroidism and cancer account for 90% of cases of hypercalcemia
Primary Hyperparathyroidism • Estimated incidence is 1 case per 1000 men and 2-3 cases per 1000 women • Incidence increases above age 40 • Most patients with sporadic primary hyperparathyroidism are postmenopausal women with an average age of 55 years
Primary Hyperparathyroid • Causes • Solitary Adenoma • Parathyroid Carcinoma (rare) • Multiple endocrine neoplasia (rare) • Hypersecretion of PTH • Hypercalcemia, • HypOphosphatemia
Hyperparathyroid - Symptoms • ~80% asymptomatic • Stones (Kidneys) • Calcium deposition and nephrolithiasis • Urinary tract obstruction • Bones • OsteitisFirosaCystica • Increased osteoclasts • Increased bone turnover • Reduced cortical bone density • Moans • Fatigue, Depression, Confusion
Hyperparathyroid – Symptoms (cont) • Other • N/V, Constipation, Polyuria • Short QT • Severe – “Parathyroid Crisis” • Renal Failure from nephrocalcinosis • Coma, Cardiac Arrest
Primary Hyperparathyroid • Diagnosis • Elevated serum PTH immunoassay (high sens), high calcium, low or normal phos (decr prox tubular reabsorption) • Elevated 1,25(OH)2D (low spec) • Imaging • 99m-technetium sestamibi • Ultrasound
Scintigraphy Images Traditional Sestamibi Sestamibi-SPECT
Primary Hyperparathyroid • Treatment • Surgical Indications • Ca > 11.5, T-score < -2.5, renal stones • Medical • Replace volume • Facilitate calciuresis (loop diuretics) • Bisphosphonates – decrease bone reabsorption. • Calcitonin • Hormonal Therapy – Raloxifene, other SERMs • Cinacalcet (not FDA approved)
Familial Syndromes • MEN I • MEN IIA • Familial Hypocalciuric Hypercalcemia • Hyperparathyroidism-jaw tumor syndrome • Fibro-osseous jaw tumors • Renal cysts • Solid renal tumors • Familial isolated hyperparathyroidism
MEN I • MEN I • 1 in 30,000 persons • Features: • Hyperparathyroidism (95%) • Most common and earliest endocrine manifestation • Gastrinoma (45%) • Pituitary tumor (25%) • Facial angiofibroma (85%) • Collagenoma (70%) • HPT in MEN I • Early onset • Multiple glands affected • Post-op hypoparathyroidism more common (more extensive surgery) • Successful subtotal parathyroidectomy followed by recurrent HPT in 10 years in 50% of cases
STIGMATA OF MEN I Lipomas Collagenomas Angiofibromas
MEN IIA (Sipple’s Syndrome) • Features: • MTC(95%) • Pheochromocytoma(50%) • HPT(20%) • RET mutation (98%) • 1 in 30,000-50,000 people • Usually single adenoma but may have multi-gland hyperplasia
Secondary Hyperparathyroid • Vit. D deficiency • Primary decreased calcium absorption in elderly • Increased phosphate in acute or chronic renal failure
Secondary Hyperparathyroid • Treatment • Phos Binders • Vitamin D analogs • negative feedback on PTH gene transcription • Limited use in setting of hypercalcemia • Cinacalcet (Sensipar)
Tertiary Hyperparathyroid • Tertiary Hyperparathyroidism is essentially secondary hyperparathyroidism that is no longer responsive to medications. • Also occurs after renal transplant, where hypertrophied glands continue to oversecrete PTH (set point alteration) • May require surgery
Signs & Symptoms • Features of Hypocalcaemia • Tetany • Depression • Perioralparaesthesiae • Carpopedalspasm-Trousseau’s sign • Cataract • Facial muscle twitch-Chvostek’s sign
Associations • Addison’s • Pernicious anaemia • Hypothyroidism • Hypogonadism
Treatment • Alfacalcidol Lifelong follow up needed