Download
1 / 58
580 likes | 600 Views
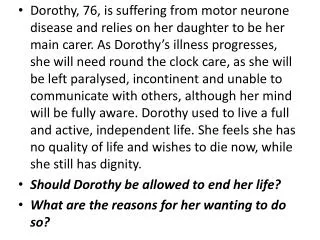
The Role Of The Hospice Medical Director In an Era of Changing Hospice Regulation. Daniel Maison, MD FAAHPM Palliative Medicine Specialist Spectrum Health System. Faculty Information. Daniel Maison, MD FAAHPM Palliative Care Physician Spectrum Health System Palliative Care/MC 120

E N D
The Role Of The Hospice Medical Director In an Era of Changing Hospice Regulation Daniel Maison, MD FAAHPM Palliative Medicine Specialist Spectrum Health System Oregon Hospice Association PPE
Faculty Information Daniel Maison, MD FAAHPM Palliative Care Physician Spectrum Health System Palliative Care/MC 120 145 Michigan Street NE, Suite #5120 Grand Rapids, MI 49503 dlmaison@yahoo.com
Objectives After attending this presentation, participants will be able to list 3 Medicare requirements for hospice physiciansAfter attending this presentation, participants will be able to discuss 3 new challenges posed by these regulationsAfter attending this presentation, participants will be able to discuss 3 strategies for overcoming these challenges Oregon Hospice Association PPE
Introduction • The Medicare regulatory landscape continues to evolve • Many new rules • Many of these new rules directly apply to hospice physicians Oregon Hospice Association PPE
How can we know what to do? • We will spend time today exploring the new regulatory demands in detail • No easy task keeping up with what is required • If we don’t understand what is required, how can we prepare for the intense level of scrutiny that is taking place? Oregon Hospice Association PPE
Some History • The new Conditions of Participation (CoPs) are the first major changes since 1983 • Hospice as a whole has changed tremendously (growth/patients served) • The government is now looking at hospice in a different way Oregon Hospice Association PPE
Changes in Hospice • Hospice has grown tremendously • Approximately a 500% increase in spending on hospice over the past few years • Expected to continue growing rapidly (doubling again in the next 10 years) Oregon Hospice Association PPE
The curse of hospice success • We are now on the RADAR of the federal government • Scrutiny has increased and will continue to do so • RAC’s and other auditing tools are part of this new level of interest Oregon Hospice Association PPE
What is driving hospice growth? • Population changing (population aging) • More acceptance of hospice • More referrals, received earlier • Kinds of patients we serve • 40% in 2006 had non-cancer diagnoses versus a time when nearly all hospice patients had cancer Oregon Hospice Association PPE
Growth Reasons (cont.) • More hospices over all • Increasing length of stay (CAP limits) • ALOS went from 62 to 82 days from 2000 to 2006 • Physician billing piece • Big increase over the past 10 years • Focus of greatly increased scrutiny Oregon Hospice Association PPE
How has Medicare reacted to this growth? • Increased oversight (CMS, OIG) • Increasingly asking questions (MedPAC) • The RAC’s • Changing the rules of the game (the new CoPs) Oregon Hospice Association PPE
So, what is MedPAC? • Medicare Payment Advisory Commission (MedPAC) • Independent government body set up in 1997 by the Balanced Budget Act • Advises Congress of how Medicare is run • Hospice is on their RADAR of late Oregon Hospice Association PPE
Some things MedPAC recently recommended • Changing the way we are paid to provide hospice services • Increasing physician oversight (before 180 days and every 60 days) • Have a look at Hospice in SNF’s and the relationships between these two entities • More data collection requirements Oregon Hospice Association PPE
The New CoPs • Went into effect December, 2008 • First major change to hospice rules since the MHB began in 1983 • Goals are to make sure hospice care is “patient centered”, get more data (QAPI, outcomes driven) • Ensuring the attending physician is part of the picture • Continuity of care is ensured Oregon Hospice Association PPE
Medical Director • There can be only one per hospice • Have to designate one person to be the medical director (not several people) • Hospices have to be able to document that this person has the wherewithal to care for hospice patients (right skills, knowledge) Oregon Hospice Association PPE
What is the Medical Director responsible for? • Supervising all of the hospice physicians • Be in compliance with all of the other rules (e.g. state laws) • Has to step up coverage if the attending physician is not available • There must be a hospice physician available at all times, 24/7 Oregon Hospice Association PPE
What are some of the other elements of the new CoPs? • We will go over some of the changes that apply to hospice in general • We will also go into more detail about physician specific issues • Remember that we are all in this together and that we are all responsible to help our organizations stay in compliance Oregon Hospice Association PPE
Pain and Symptom Management Be a participant in the the development of their own POC Choose their attending Get information about the MHB Get info about the services you can provide them Refuse any treatment Their medical information will remain confidential What is every patient entitled to according to Medicare? Oregon Hospice Association PPE
Huge Emphasis On The Initial And Ongoing Assessment Of The Patient • There are specific requirements for: • Timeframes • Content • Who should complete it • How often it needs to be updated and who does the updating • Where else the assessment needs to have cross-talk with the rest of the organization Oregon Hospice Association PPE
Initial and Comprehensive Assessment: Who completes it? • Everyone is in on the act • Initial done by an RN • Completed by the IDG (that also includes attending physician) Oregon Hospice Association PPE
Other highlights to discuss in brief • Plan of Care specifics • Coordination of Hospice Services • QAPI Oregon Hospice Association PPE
Plan of Care Specifics Highlights • Plan of care has to flow from initial and comprehensive assessments (what is identified is what is addressed and solved) • Has to reflect the goals of care we are serving • Has an intervention listed for every problem identified Oregon Hospice Association PPE
Plan of Care Specifics Highlights (cont.) • Documents everything we need to be successful for meeting a patient’s needs • Scope/Frequency of services we are to provide (how often will the patient get a visit from the hospice aide?) • Medications/Treatments/Supplies • Documented understanding of POC by patient and/or representative Oregon Hospice Association PPE
Coordination of Hospice Services • Have to be able to demonstrate communication • Have to be able to demonstrate IDT is in charge of a patient’s care (directing, coordinating, supervising) • Plan of care is driving what we are doing Oregon Hospice Association PPE
Coordination of Hospice Services (cont.) • Remember, it ALL has to flow and match up • What is identified in the initial and comprehensive assessments is what is addressed in the plan of care • The patient/family goals of care are what we are attempting to accomplish • What is discussed in IDT is what is in the POC and that you are documenting that we are addressing those issues Oregon Hospice Association PPE
Coordination of Hospice Services (cont.) • Don’t let the communication stop at the door • Make sure that we are also documenting communication/coordination with our community partners • Again, we are responsible for demonstrating that everything happening jives with our plan of care Oregon Hospice Association PPE
QAPI • Big big role under the new CoPs • It’s all about data these days • Have to pick projects, track and document • Physicians are a big part of this process • Physicians nearly had an even bigger role in the proposed CoPs (did not come to pass) Oregon Hospice Association PPE
QAPI (cont.) • Projects should focus on areas of opportunity/challenge • Have a significant impact on patient care • Have to take action based on what is found • Make sure that what you are doing is helping Oregon Hospice Association PPE
The Physician Narrative • New Requirement as of October 1st, 2009 • Must be done on EVERY patient on admission and at EVERY recertification • Must be done by the physicians themselves Oregon Hospice Association PPE
The Narrative (cont.) • The form has to indicate where the physician got the information: • A review of the medical record • Direct examination of the patient • Combination of a review of the medical record and direct examination of the patient Oregon Hospice Association PPE
The Narrative (cont.) • The narrative must contain enough information on its own to make the case why the specific patient qualifies for hospice services with a prognosis of 6 months or less if their disease runs its normal course Oregon Hospice Association PPE
What else do you need on the narrative • The physician’s signature has to immediately follow the narrative statement • If you separate the Certificate of Terminal Illness and the narrative on 2 different pages, the physician has to sign BOTH Oregon Hospice Association PPE
What won’t pass muster • Another hospice team member (e.g. nurse) completing the narrative and then having the physician sign off on it • Check boxes • Statements like: • “As Above” • “Hospice appropriate” • “Terminal” or “Patient Died” Oregon Hospice Association PPE
Remember . . . • The narrative should be able to stand on its own to make the case for hospice eligibility • Has to make the case vis á vis the LCD’s to prove eligibility • Make sure you write enough to prove your point Oregon Hospice Association PPE
Surveyors are zeroing in on narrative • If they pull a chart and the narrative is either missing, incomplete, or does not make the case, a hospice can receive a technical denial • Same as if you do not have a valid CTI or NOE • Expect scrutiny to increase not decrease Oregon Hospice Association PPE
What we are trying to do We are painting a picture as to why someone is eligible for hospice services Why are we saying that this particular patient has a prognosis of 6 months or less to live? Burden of proof is on us to demonstrate with supporting evidence why someone is eligible Be comfortable that you have the data you need to support the eligibility of every patient you admit should her chart be requested for review
Sample Physician Narrative Mrs. X has a PMH of Alzheimer’s X 10 yrs; secondary DX: dysphagia, and non-healing Stage IV decubitus on sacrum; co-morbid DX: CVA and CHF; KPS 40%; FAST 7d; dependent in 5:6 ADL’s; and “tremendous weight loss” per nursing home staff. Based on the above, I believe that the patient has a prognosis of 6 months or less if her disease runs its normal course. Remember to document the source of your information (chart review/examination of the patient/both)
What you write depends on what you are trying to prove • Very different narrative for a patient with Metastatic Pancreatic Cancer versus a patient with Dementia • Try to hit the key elements of the LCD for a patient’s hospice diagnosis • Summarize criteria in paragraph form Oregon Hospice Association PPE
For cardiopulmonary disease • Utilize NYHA classification scale • “Maximal medical management?” • Document: • O2 utilization and liter flow; pulse oximetry • Respiratory and pulse rates at rest and after any exertion; • Blood pressure; • Edema levels, if any • Hospitalizations, ER visits
COPD • Dyspnea at Rest • Frequent/Increasing ER and/or Hospitalizations • Hypoxemia at rest on room air • Right Sided Heart Failure • Resting Tachycardia • Weight Loss Oregon Hospice Association PPE
Dementia • Utilize FAST scale (7A or worse) • Utilize non-verbal pain and symptom assessment scales and/or caregiver reports; and • Weight loss • Serious Infections • Skin Breakdown • ADL dependence • KPS/PPS
How about recertification? • Same process, but hopefully will be even more straightforward • You have had this patient under your care for several months • Should be able to make your case or decision to discharge easily if you have tools in place Oregon Hospice Association PPE
Do not wait until the recert date • Use every IDG as an opportunity to discuss eligibility • Don’t make a decision the night before the benefit period is over • No recertification decision should ever be a surprise Oregon Hospice Association PPE
FI/RHHI nuance • The LCD’s are FI/RHHI (Regional Home Health and Hospice Intermediary) specific • Become intimately familiar with your local areas requirements • Much in common across the country, but make sure you know your specific ones well Oregon Hospice Association PPE
Make it easy for them to say “Yes” • Remember auditors are busy too • They are reviewing many charts and have to wade through a lot of data • Help them glean what they need to make their decision • Make every chart reviewed a “no-brainer” Oregon Hospice Association PPE
Example Summary • Mr. Jones is an 82 year old gentleman with a history of end stage, oxygen-dependent COPD. He has been hospitalized 3 times in the last six months, has lost more than 10% of his body weight in the last 6 months, and has a bed to chair existence. Oregon Hospice Association PPE
Sample Summary (cont.) • He has evidence of right-sided heart failure as evidenced by JVD and intractable lower extremity edema. His heart rate is 104 at rest. • Based on the all of the above, this patient clearly has a prognosis of 6 months or less to live if his disease runs its normal course. Oregon Hospice Association PPE
“As evidenced by” • Again make it easy • Can’t just say “The patient is declining” • Define “decline” • “The patient continues to decline as evidenced by progressive symptoms, increased weakness, and continued weight loss.” Oregon Hospice Association PPE
For those patients that have been on longer than 6 months • What is coming January 1st, 2010 • Have to have a face to face meeting with every patient 15 days or less prior to end of 2nd 90 day certification period • NHPCO released commentary via email regarding rule on September 14th, 2010 Oregon Hospice Association PPE
Some tools to consider • What forms do you use to gather data on the hospice patients evaluated for admission? • Make it easy for the nurses to gather what is needed for hospice physician to make a decision • A little up front work will go along way Oregon Hospice Association PPE