Download
1 / 30
540 likes | 2.72k Views
TOXOPLASMOSIS. Dr. S.GOPALAKRISHNAN. M.D Asst. Prof. Govt. Hospital for Thoracic Medicine Tambaram. INTRODUCTION. Toxoplasma Gondii is worldwide in distribution. Most common Chronic infection with Obligate intracellular Protozoan in Humans.

E N D
TOXOPLASMOSIS Dr. S.GOPALAKRISHNAN. M.D Asst. Prof. Govt. Hospital for Thoracic Medicine Tambaram.
INTRODUCTION • Toxoplasma Gondii is worldwide in distribution. • Most common Chronic infection with Obligate intracellular Protozoan in Humans. • 3-4 % of all Patients with AIDS may develop CNS Toxoplasmosis at some stage. • Greatest incidence when CD4 < 100 cells/mm3 • Decrease in CMI in chronically infected at risk of reactivation of infection.
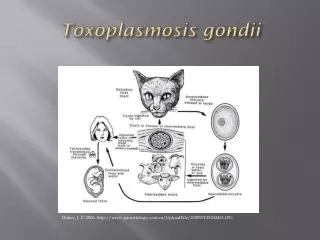
EPIDEMIOLOGY • Definite Host – CAT Sexual Cycle----Oocyst • Intermediate Host– Human,Mouse,Pig,Sheep. Asexual Cycle----Tissue cyst
EPIDEMIOLOGY • Transmission to humans • Oral • Ingestion of under cooked Pork or Lamb meat –tissue cyst. • Exposure to oocysts • Ingestion of contaminated vegetables • direct Contact with cat feces. • Others • Transplacental. • Blood Product Transfusion. • Organ Transplantation.
PATHOGENESIS ORAL INGESTION TACHYZOITE (INVASIVE FORM) DISSEMINATES THROUGH OUT THE BODY INFECTION ->ANY NUCLEATED CELL->MULTIPLICATION -> CELL DESTRUCTION -> NECROTIC FOCI -> SURROUNDING INFLAMMATION TISSUE CYST LIFE LONG CHRONIC INFECTION ONSET OF CMI
SUSCEPTIBILITY – MECHANISM IN HIV • Depletion of CD4 T cells • Decreased production of IL-2 ,IL-12,IFN-g • Decreased cytotoxic T-lymphocyte activity.
CLINICAL PRESENTATION Immuno compromised Cerebral • Manifests primarily as toxoplasmic encephalitis • Altered mental status – 75 % • Focal Neurological deficit – 70 % • Motor weakness • Speech Disturbances • Cranial Nerve Palsy • Movement Disorders • Visual Field Defects • Sensory ,Cerebellar Dysfunction
Cont… • Head ache – 56% • Fever – 45% • Seizures – 30% Extra Cereberal Ocular • Choreoretinitis – Less common than CMV Lesions adjacent to disc, old scar Multi focal, bilateral lesions typically more confluent, thick, opaque. • Anterior Uveitis
Cont… Pulmonary • Highly Lethal sepsis like syndrome • Difficult to distinguish from Pneumocystis cari. pneumonia Cardiac • Asymptomatic • Cardiac tamponade • Biventricular Failure
IMMUNOCOMPETENT • LYMPHADENOPATHY Common – CERVICAL (Single or Multiple non tender,Discrete) Generalized – 20-30% • Fever,Myalgia,Rash , Meningo-Encephalitis. • Rare: Pneumonia,Myocarditis,Polymyositis.
DIAGNOSIS * Serology Anti-IgG Antibodies • Peaks within 1-2 months after infection. • Remain elevated for life. • False negative 10-15% • Sabin-feldman dye test-gold standard • IFA-indirect • Elisa
Cont… • IgM Anti-body tests • Double sandwich Elisa • IFA • Immunosorbent agglutination assay (IgM-ISAGA)
SEROLOGY To diagnose – recent infection • Serial specimens at 3 weeks apart-4 fold increase in IgG titre. OR • Elevated IgM, IgA or IgE titres with differential agglutination test. • Useful to Identify - HIV at risk of developing toxoplasmosis. 97%-100% HIV with toxo –encephalitis have anti IgG anti bodies.
CSF • Non specific • Mild cell count – mononuclear, protein • Intrathecal Anti IgG antibodies production • Ratio > 1 supports the diagnosis of toxoplsmic encephalitis • Wright – Giemsa stain of CSF
DNA • POLYMERASE CHAIN REACTION (PCR) • CSF – Sensitivity 50 – 60% - Specificity 100% • Bronchoalveolar lavage fluid • Vitreous and aqueous humor • Blood samples – low sensitivity: toxo.encpha. • Amniotic fluid • Culture – Time consuming
NEURORADIOLOGIC STUDIES C T • Multiple, bilateral, hypodense, contrast-enhancing focal brain lesions – 70 to 80% • Lesions – basal ganglia, hemispheric corticomedullary junction. • Contrast enhancement often with ringlike pattern
MRI • More sensitive than CT • Identify more lesions than seen on CT, new lesions not seen on CT NEWER IMAGING TECHNIQUES 201T1SPECT: Thallium 201 single- photon emission computed tomography 18F FDG – PET: Fluoride 18 - Flouro – 2 deoxyglucose positron emission tomography.
DEFINITE DIAGNOSIS • Excisional Brain Biopsy: • Usually not performed • Reserved for patients who fail to respond to therapy
DIFFERENTIAL DIAGNOSIS • Primary CNS Lymphoma • Mycobacterial infections • Cryptococcal meningitis • Herpes simplex encephalitis • PML • CMV infection • Infectious mononucleosis
MANAGEMENT IN HIV • Therapy empiric in most cases • Neurologic response • 51% by day 3 • 91% by day 14 • Neuroradiologic study repeated 2-4 weeks after initiation of therapy
Cont… • Acute Therapy • Maintenance Therapy (Secondary Prophylaxis) • Prevention (Primary Prophylaxis) • Discontinuation of Prophylaxis
ACUTE THERAPY • Preferred • Pyrimethamine 200mg po loading dose followed by 75-100 mg po qd plus folinic acid 15-20 mg po qd plus sulfadiazine 1-1.5g po q6h - 6 weeks. • Alternatives • Pyrimethamine with folinic acid (as standard) with one of the following: • Clindamycin 600 mg po q6h • Clarithromycin 1g po bid • Azithromycin 1.2-1.5g po qd • Dapsone 100mg po qd - 6 weeks
MAINTENANCE THERAPY • Preferred • Pyrimethamine 25 mg po qd & folinic acid 10 mg po qd and Sulfadiazine 500-1000 mg po q 6h • Alternative • Pyrimethamine 25 mg po qd & folinic acid 5-10 mg qd po & Clindamycin 300-450 mg po q6-8h. • Atovaquone 750 mg po bid
PREVENTION • To eat well cooked meat - internal temperature of 1160C, or no longer pink inside. • Proper hand washing. • Fruits and vegetables should be washed prior to consumption. • To avoid contact with materials contaminated with cat feces, handling cat litter boxes. • To wear gloves during gardening.
Cont… • Recommended • T gondii - Seropositive patients with CD4 T cell counts <100 regardless of clinical status. • Patients with CD4 T cell counts <200 if an opportunistic infection or malignancy develops. • Trimethorprim / sulfamethazole 1 ds tab po qd • Dapsone 50 m po qd & pyrimethamine 50 mg po q week plus & folinic acid 25 mg po q week
DISCONTINUATION OF PROPHYLAXIS • CD4 T cell counts increase to more than 200 over a period of 3- 6 months in response to HAART • Restarting prophylaxis in patients CD4 T cell counts decrease to < 200