Download
1 / 40
400 likes | 580 Views
Immune Profiling in Renal Transplantation: Biopsy Correlations with Urine and Plasma PCR Studies. Surya V. Seshan, T. Muthukumar, D, Dadhania, M. Suthanthiran Weill Cornell Medical College New York-Presbyterian Hospital New York, USA. Renal Dysfunction in Transplants. Tubulo-interstitial.

E N D
Immune Profiling in Renal Transplantation: Biopsy Correlations with Urine and Plasma PCR Studies Surya V. Seshan, T. Muthukumar, D, Dadhania, M. Suthanthiran Weill Cornell Medical College New York-Presbyterian Hospital New York, USA
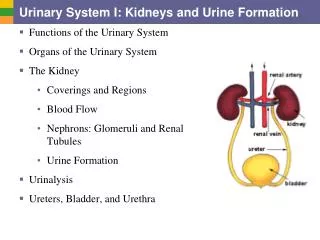
Renal Dysfunction in Transplants Tubulo-interstitial Acute Rejection • Acute tubular injury • Drug toxicity • Infections – viral, bacterial • Allergic interstitial nephritis • Perioperative or post-operative complications Vascular Chronic T cell Antibody mediated
Banff 07 Update: Diagnostic Categories for Renal Allograft Biopsies • 1 – Normal • 2 – Antibody Mediated Changes • C4d deposition with no morphological e/o active rejection • Acute AMR • Chronic AMR • 3 – Borderline Changes – suspicious for acute T cell mediated rejection • 4 – T cell Mediated Rejection • Acute • Chronic active (Chronic allograft arteriopathy) • 5 - Interstitial Fibrosis & Tubular Atrophy NOS • 6 – Others • Chronic hypertension • Calcineurin inhibitor toxicity • Chronic obstruction • Bacterial pyelonephritis • Viral infection K Solez Am J Transplant 2008
Limitations of Renal Biopsy Specimen adequacy Banff 1997 – 9-11 glomeruli, 1-2 arteries Need for the presence of cortex Patchy distribution of disease Borderline lesions Prior treatment Chronic parenchymal scarring
Immune Profiling in Renal Transplantation • Diagnosis • Therapeutic decision making • Acquire prognostic information • Monitor/surveillance of allograft function • Elucidate pathogenetic mechanisms and molecular pathways of cell activation and tissue injury Samples used: Blood, urine and tissue
Levels of Monitoring Initiating Event End Point Molecular Histological Biochemical Clinical
Methods of Immune Profiling • Immunohistochemistry Immunofluorescence Immunoperoxidase • Polymerase chain reaction (PCR) studies Viral proteins Inflammatory cells Immune mediators • Tissue Microarray studies- cDNA, Oligonucleotide • Serum and urine proteomics • Allo-antibodies – Cell & soluble ag based
Acute T Cell Rejection : Molecular events Invitation: IP10 Contact: CD103 Induced suicide: Granzyme B/ Perforin Collateral Protection: PI-9 Damage control: FoxP3
Pre-Amplification Enhanced Kinetic Quantitative (RT) PCR Assay: Designed & Validated at Suthanthiran Laboratory Design of gene specific primers & fluorogenic probes Step 1: 10 cycle PCR with multiple primer pairs of interest Step 2: Kinetic quantitative PCR with single primer pair & probe A standard curve is generated cDNA quantity expressed as copies/ ug total RNA 50 cc urine sample Centrifuge - Pellet Total RNA isolated - RNA quantified Quality checked Reverse transcribed to cDNA cDNA concentration: 1µg/100µl TE buffer Approx: 1-2 ug cDNA (cf. Biopsy 5-10 ug, Blood 10-15 ug) Urine Cells DNA mRNA cDNA Exon 1 Exon 2 Exon 1 Intron Exon 2 Exon 1 Exon 2
Non-Invasive Detection of Renal Allograft Inflammation: mRNA Profiling for IP-10 & CDCR3 in Urine Cells – Invitation genes Tatapudi RR et al, Kidney Int 2004
Immunohistochemical Localization of IP-10 and CXCR3 in Renal Allografts Tatapudi RR et al, Kidney Int 2004
Acute Allograft Rejection: mRNA Profiling of Urinary Cells for CD103 – Contact gene Ding R et al, Transplantation 2003
Acute Allograft Rejection: mRNA Profiling of Urinary Cells for Perforin and Granzyme B. They have a high degree of accuracy in distinguishing AR from other causes of allograft dysfunction The ‘Suicide Inducer’ Genes in Acute Rejection Li B NEJM 2001, Muthukumar T Transplantation 2003
Acute Cellular Rejection CD3 Gr-B TIA
Tissue Microarray and Proteomic Analysis in Acute Cellular Rejection
DNA Microarray Profiling Showing Molecular Heterogeneity in Acute Renal Allograft Rejection Sarwal M et al, N Eng J Med 2003
Proteomics Blood, urine & Biopsy tissue Surface enhanced or Matrix assisted Laser desorption Mass Spectroscopy
Proteomic Based Detection of Urine Proteins Associated with Acute Renal Failure Schaub S et al, J Am Soc Nephrol 2004
Micro RNA transcripts in renal transplants can identify acute rejection Anglicheau D et al PNAS 2009
Micro RNA in renal transplants Anglicheau D et al PNAS 2009
Antibody Mediated Rejection C4d Positive PTC Fluctuations in DSA levels Variability in C4d staining Abs to HLA Class I & II Non MHC ags in endothelium ABO Other
ENDOTHELIAL GENE EXPRESSION IN KIDNEY TRANSPLANTS WITH ALLOANTIBODY INDICATES ANTIBODY-MEDIATED DAMAGE DESPITE LACK OF C4D STAINING Sis et al. AJT 2009
Clustering endothelial transcripts detects C4d negative samples with increased endothelial transcript expression Red: high expression Blue: low expression Population= 165 biopsies with or without circulating Ab Cluster with high expression • This heatmap indicates: • All C4d+ ABMR biopsies (black) have high Endothelial transcript expression • There are also C4d negative biopsies with high expression which Ab+ (blue) or Ab negative (gray) Sis et al. AJT 2009
Acute Rejection vs. Urinary Tract Infection: mRNA Profiling of Urinary Cells for Granzyme Dadhania D et al, Transplantation 2003
CD20 Pyelonephritis in Renal Allograft CD3 Granzyme B
Graft Loss is a Significant Risk in Individuals with BKV Nephropathy INCREASED FIBROSIS and INFLAMMATION Drachenberg et al. AJT 2
Decoy cells – ground glass intranuclear viral inclusion bodies Molecular Evaluations Current Non-Invasive Diagnostic Tools Pathology Evaluations – Decoy cells, EM contrast • PCR Amplification of DNA or cDNA • Blood • Urine EM of negatively stained urine sample Icosahedral spherical shape of 40nm Urine Haufen Urinary Haufen – cast like viral aggregates
BKV (Polyoma virus) Associated Nephritis • BKV nephritis is often associated with histological findings consistent with acute rejection such as mononuclear infiltration and tubulitis • In the setting of BKVN, management decisions are contingent upon accurate differentiation from acute allograft rejection (AR). • Differentiation of BKV nephritis from concurrent rejection process • Considerable tubulitis - C4d staining • Vascular rejection - HLA –DR expression
BKV Nephritis: mRNA Profiling in Urinary cells for Granzyme B • Urinary cell Granzyme B mRNA (a cytotoxic attack molecule) levels, but not BKV VPI mRNA levels are a correlate of allograft damage in patients with BKV nephritis (as defined by the presence or absence of tubulitis). • (Manuscript under preparation) • Allograft failure in patients with BKV nephritis can be predicted by urinary gene expression profiles.
Active tubulo-interstitial inflammation in BKV nephritis case Gr-B HLA-Dr
Conclusions • Real Time Quantification of Urinary Cell mRNA levels allows for • accurate diagnosis of BKVN • allows for measurement of prognostic markers simultaneously • Individuals with increased levels of cytotoxic T cell molecule, granzyme B, have initial higher levels of creatinine and increased risk of subsequent decline in renal allograft function. • Whether elevated levels of granzyme B reflect adaptive immune response against BK virus or against the allograft or both remains to be determined, thus modifying the management of BKVN. (Manuscript in preparation)
Genomics/Proteomics/PCR vs. Histopathology Molecular screening may be an attractive alternative for immune surveillance and early diagnosis of acute rejection These advanced molecular studies could have a potential for a more objective and quantitative assessment of allograft immune response as well as differentiate from other forms of allograft dysfunction. Considering the limitations of the biopsy tissue, significant reduction in the sources of variability can be achieved. Such data may complement the routine histological examination in the grand scheme of immune profiling in renal transplantation
Special thanks to the urine gene expression group in Suthanthiran Laboratory C Chang R Ding M Lagman V Sharma B Li C Snopkowski Thank You