Download
1 / 46
760 likes | 1.55k Views
Infections in Pregnancy. Max Brinsmead MB BS PhD March 2014. Rubella Infection. Caused by the pleomorphic RNA virus of the genus Rubivirus Infects only human subjects In adults and children causes: Mild fever & malaise Generalised fine erythematous rash – rarely purpuric

E N D
Infections in Pregnancy Max Brinsmead MB BS PhD March 2014
Rubella Infection • Caused by the pleomorphic RNA virus of the genus Rubivirus • Infects only human subjects • In adults and children causes: • Mild fever & malaise • Generalised fine erythematous rash – rarely purpuric • Cervical lymphadenopathy • Arthralgia
Rubella in a Pregnant Woman • Before 12 weeks pregnancy • Miscarriage • Cardiac anomalies • Nerve deafness • Cataracts or retinopathy • Mental retardation • Fetus somewhat safer in the 2nd trimester but… • In the second half of pregnancy • Hepatosplenomegaly • Failure to thrive, osteitis • Diabetes, hypothyroidism and GH deficiency • Progressive panencephalitis = The Congenital Rubella Syndrome
Prevention of Congenital Rubella • Immunise all children at 12 -15m (MMR) • Test all women who are pregnant (or plan to conceive) for immunity • Avoid infection if pregnant • Spread by nasopharyngeal droplets +/- 7 days from the time of rash • Retest any pregnant woman who is exposed to the virus • Terminate pregnancy for proven infection • Immunise women postpartum if low titre or non immune • Immunisation of a pregnant woman with the live virus is not recommended but is also not associated with teratogenesis
Varicella • Caused by Herpes zoster • Causes • Chickenpox • Shingles • Fetal varicella syndrome (FVS) • In pregnancy maternal risks of pneumonitis (10%) are greater than the fetal risks of FVS (2%)
Fetal Varicella Syndrome • Greatest risk is maternal infection 13 – 20w • Mental retardation 50% • Skin scarring • Eye defects (micropthalmia, chorioretinitis and cataracts) • Limb hypoplasia • Bowel/Bladder dysfunction • Intrauterine diagnosis requires fetal blood sampling for HZV PCR
Neonatal Varicella • Risk is greatest if maternal rash occurs 5 days before delivery and up to 2 days after • Transmission rate 20 – 60% • 30% neonatal mortality if untreated • Acyclovir recommended
Maternal Varicella in Pregnancy • Pneumonitis 10% • Hepatitis • Encephalitis • Acyclovir or similar required
Recommendations • Prenatal screening and/or Immunisation • Serum HZV IgG at the 1st antenatal visit* • ZIG for non immune women who come into close contact with Varicella • Prophylactic oral Acyclovir for exposure >20w • Delay delivery >5 days after rash • Neonatal ZIG and Acyclovir for high risk neonate • Immunise health care workers • Exclude those non immune to Varicella from care of pregnant women for 8 – 21days after possible infection
Genital Herpes • 66% caused by H. simplex Type 2 • 33% associated with H simplex Type 1 • Is a latent and recurrent infection in up to 1:5 adults • ~1:50 women have this virus during pregnancy • But most are secondary (or recurrent) infections • Even if the woman says she has never had it before
Neonatal Herpes • Three subgroups of neonatal infection • Skin, eye and mouth disease • Encephalitis only • Disseminated disease • Disseminated disease has 80% mortality (untreated) and 30% with antiviral agents • And 1:5 risk of long term morbidity in survivors • Risk of death from skin, eye and mouth disease is 2%
Maternal Herpes • Primary infection can be disseminated with encephalitis, hepatitis and skin eruptions • Is more common in pregnancy because of the mild immunosupression which occurs • Most infections during pregnancy are secondary • But recurrences are more common because of pregnancy-related immunosupression
Vertical Transmission of Herpes • Mostly occurs when the fetus contacts infected genital secretions • But intrauterine infection and FDIU possible • Neonatal infection is also possible • Disseminated Herpes occurs after primary maternal infection • Often with premature delivery • Secondary maternal Herpes can cause • Skin, eye and mouth disease • And sometimes isolated neonatal encephalitis • Because maternal antibodies do not protect the brain
Risk of Vertical Transmission • With maternal primary Herpes the risk of neonatal infection is 26 – 56% • With maternal secondary Herpes the risk of neonatal infection is 1 – 3%
Diagnosis of Genital Herpes • Often unrecognised in its recurrent form • Typically localised pruritis and pain • Blister and ulceration • PCR is a sensitive and specific test if appropriate material is collected • Serum IgG and IgM can be useful in distinguishing primary and secondary infection • Viral culture
Why Caesarean Section? A prospective study of 58,000 women in Washington USA identified 202 of whom 117 delivered vaginally and 85 by CS. The risk of neonatal sepsis was reduced by 86% by CS but the RR confidence intervals were wide (0.02 – 1.12) This means that it would require 1583 Caesarean sections of patients with secondary Herpes to prevent one case of neonatal Herpes (with mortality or morbidity)
Maternal Secondary Herpes • Weekly cultures are not predictive • Daily Acyclovir from 36 weeks reduces the risk of • A recurrence at the time of delivery • Asymptomatic virus shedding • The chance of CS • And should be offered to women who would elect CS if there was a Herpes outbreak at the time of labour
Herpes visible at the onset of labour • If thought to be a secondary infection then CS is not mandatory • Requires patient counselling and her choice should be respected • If there are ruptured membranes then delivery should be expedited • Fetal trauma should be avoided • The neonatal service should be alerted
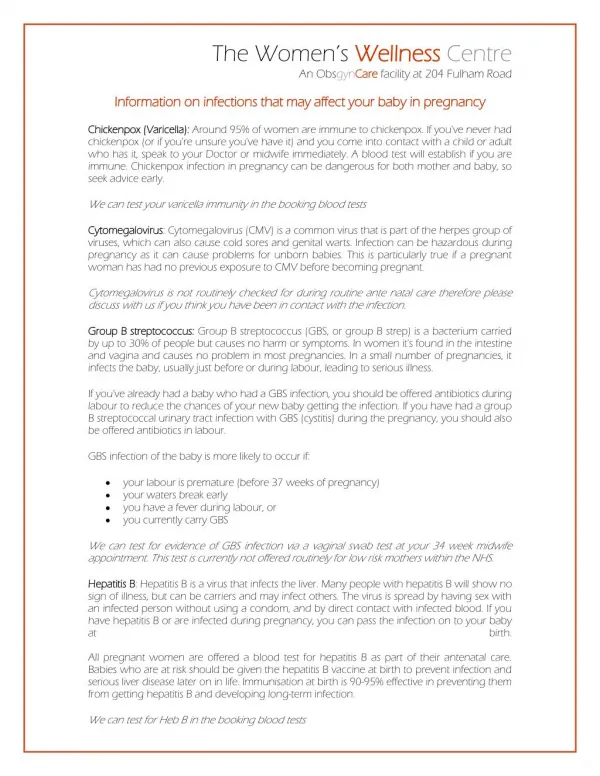
Cytomegalovirus • Proper name is Human Herpesvirus 5 • 1:100 babies are born with this congenital infection • 1:10 of those infected will show some effect • 1:10 of those will have severe mental retardation • CMV is a common cause of mental retardation • And causes 30% of congenital neural deafness • ~40% of women are non immune when pregnant • Health workers and women with children who bring home CMV are most at risk • Vaccination is not possible • But trials are currently in progress
Neonatal CMV Syndrome • Small for dates • Failure to thrive • Hepatospenomegaly • Microcephaly • Cerebral calcifications • Chorioretinitis • Hearing deficits (may occur later in life) • The virus can be detected in urine and saliva
Vertical CMV Transmission • 1-4% of women seroconvert during pregnancy • 90% of congenital CMV is due to primary maternal infection • Risk to the fetus with CMV reinfection is 0.5 – 2% • Reinfection with another strain is also possible • The earlier the infection in pregnancy the greater the risk • Can cause miscarriage in the 1st trimester • Risk to the fetus is small if infection is acquired prior to pregnancy • Fetal infection cannot be predicted by maternal testing • but IgG avidity testing emerging as a pointer
Treatment of Intrauterine CMV • Termination of pregnancy is really the only option • Should respond to anti viral agents such as Ganciclovir and Valganciclovir but their role in pregnant women and the neonate is unproven • Trials are underway • Likewise little data on the role of prophylactic immune gamma globulin • One non-RCT trial showed it to reduce fetal risk by ≈60%
Parvovirus • Caused by Parvovirus B19 • Causes epidemic Fifth Disease or “Slapped Cheek Syndrome” in pre school children. • When intrauterine infection occurs it affects haemopoeisis. This results in fetal anaemia and hydrops fetalis. • However, recovery is usually spontaneous and complete and there are no long term sequelae
Vertical Parvovirus Transmission • 50-66% of pregnant women are Parvovirus immune • Most infections occur from the mother’s own pre school child • Spread by droplets c sneezing, coughing • Incubation period is 4 -14 days • Rash occurs on the face but also on hands, wrists & knees • Maternal symptoms include polyarthalgia, fever and non specific rash
Fetal Risk • Transplacental transmission rate is ~30% • Can cause hepatitis and myocarditis • 20% risk of fetal death in the 1st trimester • Causes about 3% of miscarriages • Risk of hydrops is greatest in the second trimester • When a fetal death rate of about 15% • But by 20w the risk of fetal death has fallen to 6%
Treatment of Intrauterine Parvovirus Infection • Termination of a pregnancy is not required • Weekly ultrasound monitoring for signs of hydrops and middle cerebral Dopplers may be undertaken after documented evidence of maternal infection • But most affected fetus will recover spontaneously • A small number may require intrauterine transfusion for severe anaemia • This is ~85% successful
Toxoplasmosis • Caused by the protozoan parasite Toxoplasma gondi • Is endemic in most societies • And the definitive host is cats • Has a complex life cycle but infectious oocysts can live for many months in soil • 10 – 25% of adults have serologic evidence of previous infection • In most it causes a mild illness with fever, malaise and lymphadenopathy • But transplacental infection can cause congenital disease
Congenital Toxoplasmosis • Mental retardation • Learning difficulties • Cerebral calcifications • Chorioretinitis blindness • Hydrocephalus • Epilepsy
Vertical Transmission • 50% of congenital Toxoplasmosis is due to eating contaminated meat, mostly pork • Remainder to to contact with cats’ faeces or contaminated soil • ~1:200 women will become infected during pregnancy • Of these ~1:10 will deliver a baby with congenital Toxoplamosis • Infection in early pregnancy is less likely to cross the placenta • But this has more serious effects when it does
Treatment • Acute infections can be treated with Spiramycin or sulphadiamine/pyrimethamine • This will reduce the risk of vertical transmission by ~50%
Preventing Congenital Toxoplasmosis Pregnant women should: • Cook meat thoroughly and check core temperature with a cooking thermometer • Prevent contamination of food by uncooked meat • Avoid contact with cat faeces • Wash or peel vegetables and avoid contact with soil
Listeriosis • Caused by Listeriamonocytogenes • A motile Gram-positive bacterium • Relatively ubiquitous in the environment • Found in 1 – 15% of human faeces • Infection in animals is common • Human infection is rare except: • When immunocompromised • Pregnant • Elderly • Newborn
Listeriosis in Pregnancy • Fewer than 10 per 100,000 women • Infection may be asymptomatic • But the following symptoms also occur: • Fever (38.2 to 41.20 C and mean of 38.9) • Malaise • Flu-like symptoms such as headache and myalgia • Rarely CNS infection with meningitis or abscess • Transmission risk to the fetus about 50% • Untreated the risk of fetal death is 20 – 30% • Pathognemonic finding is widespread abscesses & granulomas in the fetus (rare)
Treatment • Use Ampicillin 2G every 6 – 8 hrs • This high dose is recommended in order to cross to the amniotic fluid and membranes in sufficiently high concentrations • For penicillin allergy use Bactrim/Septrim • Sometimes Vancomycin
Prevention • Aims to reduce a pregnant woman’s exposure to possible contaminated food sources • Authorities recommend dietary advice to ALL pregnant women • But this has never been tested by RCT
Typical Pregnancy Advice “Listeria is a very rare infection that is mild in a mother but can be fatal to the baby in utero. You should NOT eat the following: • Unpasteurised milk products esp. Soft cheeses, included feta, Brie, Camembert and ethnic-style cheeses. (Hard cheeses, pasteurised, cottage & cheese spreads are okay) • Raw seafood • Uncooked meats and vegetables • Cold-stored cooked meats and pates, • Milk products stored at >40 C • Beware of cross contamination from these sources • Wash all fruit and vegetables • Cook foods at recommended temperatures”
Group B Streptococcus • Group B Streptococcus is the most frequent cause of severe neonatal infection within 7 days of birth • Incidence 0.5 – 1.5 per 1000 • Risk of death is 10 – 30% • And there is also morbidity in survivors • 15 – 30% of pregnant women are carriers of GBS (Varies with climate) • 50% of their infants will become colonised during birth and • 1 – 2 % will develop sepsis • Intrapartum antibiotics significantly reduces the rate of neonatal GBS sepsis
Possible strategies • Identify and treat high risk patients – no screening • UK (unchanged view in 2012) • Screen all and treat all GBS carriers • USA and many Australian hospitals • Screen all and treat only those with additional risk factors • Canada
Is Screening effective? • There are no RCTs • Observational studies show that intrapartum antibiotics reduce the risk of neonatal GBS sepsis by 50 – 95% • Meta analysis says 86% • Rate of GBS sepsis fell by 33 – 70% in the US after introduction of universal screening
Is the treatment safe? • There are no RCTs • Some 15 – 30% of all women require treatment • You have to treat 714 women to prevent one case of neonatal sepsis • And 7000 women to prevent one neonatal death • Risk of fatal maternal anaphylaxis 1:100,000 • This means one maternal death for every seven (7) babies saved • Unknown risks from non-fatal anaphylaxis • Unknown problems from antibiotic use
HIV in Pregnancy • Risk of maternal death is increased 6-fold • Concurrent infections including TB • All obstetric causes • Increased risk of poor obstetric outcome • Miscarriage • Stillbirth • Pre term birth • IUGR • Mother to Child transmission (MTC) of HIV • Is the most common means of HIV transmission in the world • Risk is 25 – 50%
HIV Mother to Child Transmission • 80% occurs during labour • Can be reduced by 50% Caesarean section before membranes rupture • But only used where CS is safe in the short and long term • And viral load is >1,000 ml/plasma • A better option is maternal HAART (Highly active anti-retroviral therapy • If mother receives triple therapy from <28w, has elective CS & does not breast feed MTCT is 1-2%
Current WHO Guidelines • All pregnant women should be tested for HIV • All HIV patients to begin HAART asap • Continue right through VAGINAL DELIVERY • Tail off non-eligible mothers from therapy after they have stopped breast feeding AND • Give the infant oral NVP whilst ever mother is breastfeeding plus one week (up to 12 months) • Mothers eligible to continue triple therapy to continue whilst breast feeding PLUS • Give the neonate 6 weeks of AZT and NVP for as long as the mother is breast feeding • It is hoped that MTC will be 1-2%
Syphilis in Pregnancy • Typically does not cross the placenta until >20 weeks • Fetal effects include… • Stillbirth • Intrauterine growth restriction • Prematurity • Neonatal effects include… • Hepatosplenomegaly • Pneumonia • Anaemia & Jaundice • Skin lesions • Osteochondritis
Treatment of Syphilis • For a mother with proven active Syphilis • Give 3 doses of Benzathine penicillin 2.4 mU weekly • Erythromycin 500 mg 4 x daily for 15 – 30 days for true penicillin allergy • For a neonate • 25,000 IU/Kg Penicillin twice daily for 10 days • Follow up and treat the sexual partner
What is the TORCH test • TORCH is an acronym commonly used in the evaluation of stillbirth, IUGR or neonatal failure to thrive • T = Toxoplasmosis • O = Other (includes HIV, Syphilis etc) • R = Rubella • C = Cytomegalovirus • H = Herpes (simplex and varicella • Typically serum IgG and IgM for these infections repeated after 3w but of limited use