Download
1 / 45
460 likes | 754 Views
The Therapeutic Use of Reclast® (zoledronic acid) in Paget’s Disease of the Bone. Stephanie Piemontese PharmD Candidate 2010 University of Pittsburgh School of Pharmacy. Objectives. Normal Bone Physiology. Bone has both structural and metabolic properties

E N D
The Therapeutic Use of Reclast® (zoledronic acid) in Paget’s Disease of the Bone Stephanie PiemontesePharmD Candidate 2010University of Pittsburgh School of Pharmacy
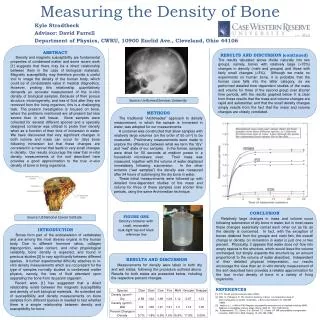
Normal Bone Physiology • Bone has both structural and metabolic properties • Structural: locomotion, respiration, and protection • Metabolic: storage of Ca++, Phos, and carbonate; H ion buffering, bind toxins and heavy metals • Bone is made up of collagen and mineral components • Collagen gives flexibility and energy-absorbing capability • Mineral component gives stiffness and strength
Two types of bone: cortical and trabecullar • Cortical bone’s major function strength/protection • Trabecular bone is more metabolically active • fjfj
Paget’s Disease of the Bone • Non malignant disease involving accelerated bone resorption followed by deposition of dense, chaotic, and ineffectively mineralized bone • Differs from osteoporosis by the involvement of discrete sections of bone remodeling • Schneider, Dipiro
Aside from osteoporosis Paget’s is the most common bone disorder • Equally prevalent in men and women • Increased incidence in persons > 50 yo • 3% US population affected • Schneider
Clinical Features Schneid, Dum • Can affect any area • Most commonly involves axial skeleto • Usually affects at least 2 bones • Can be symptomatic of asymptomatic • Most common symptom is pain the affected bone
schn • Complications include: Neurologic, hearing, vision, cardiac, and oncologic
Occurs in 3 phases (Schneider) • Intense osteoclastic activity and bone resorption • Osteoblastic phase producing woven bone, with ineffective mineralization • Dense cortical and trabecullar bone deposition
Etiology schle, dum • Viral and hereditary causes • Particles contained in osteoclasts of Pagetic bone appear to be paramyxovirus nucleocapsids
Reclast® (zoledronic acid) • Approved by the FDA in 2001 • A bisphosphonate approved for: • Treatment of osteoporosis in postmenopausal women • Prevention of osteoporosis in postmenopausal women • Treatment to increase bone mass in men with osteoporosis • Treatment and prevention of glucocorticoid-induced osteoporosis in patients expected to be on glucocorticoids for at least 12 months
Indication for Paget’s Disease • Indicated for treatment of Paget’s disease in both men and women • Indicated in patients with elevations in serum alkaline phosphatatse of > 2 times higher than upper limit of age-specific normal rangesOR • Those who are symptomatic OR • Those at risk for complications from their disease
Dosage and Administration • A single 5mg infusion given IV over no less than 15 minutes • 1500mg elemental calcium and 800 IU vitamin D daily • Administer through a separate vented infusion line • Avoid contact with any calcium or divalent cation-containing solutions • Patients must be appropriately hydrated prior to administration • Acetaminophen administration following Reclast administration may reduce incidenc of acute-phase reaction symptoms
Retreatment of Paget’s Disease • After a single treatment with Reclast and extended remission period is observed • Specific re-treatment data are not available • However, can be considered in patients who have relapsed based on serum alkaline phosphataseOR • In those patients who failed to achieve normalization of their serum alkaline phosphatase levelOR • In symptomatic patients as dictated by medical practice
Mechanism of Action • Class: bisphosphonate • Acts primarily on the bone • Inhibitor of osteoclast-mediated bone resorption • High affinity for mineralized bone
Contraindications • Hypcalcemia • Hypersensitivity to any component
Warnings and Precautions • Reclast® ≠ Zometa® • Hypocalcemia and Mineral Metabolism • Renal Impairment • Osteonecrosis of the Jaw (ONJ) • Pregnancy • Musculoskeletal Pain • Patients with Asthma
Adverse Reactions • Most common ADR (>10%) were pyrexia, myalgia, headache, arthralgia, pain in extermities • Other clincially important ADR were flu-like illness, nausea, vomiting, diarrhea, eye inflammation, hypocalcemia, hypophosphatemia, ONJ, acute renal impairment, allergic reactions
Drug Interactions • Aminoglycosides • Loop diuretics • Nephrotoxic drugs • Drugs primarily excreted by the kidney
Use in Specific Populations • Pregnant and nursing mothers – should not receive Reclast • Pediatric use – not indicated • Geriatric use – monitor renal function • Renal Impairment – should not be used <35mL/min • Hepatic Impairment – no data
Pharmacodynamics • Treatment with a 5mg annual dose of Reclast reduces bone turnover markers to the pre-menopausal range with an approxiamte 55% reduction • Serum beta-C-telopeptides = bone resorption • Bone specific alkaline phosphatase & serum N-terminal propeptide of type I collagen = bone formation • Progressive reduction of bone turnover with repeated annual dosing
Pharmacokinetics • Distribution • Triphasic process • t/2α=0.24hrs, t1/2β=1.87hrs, t1/2γ=146hrs • Protein binding ranges from 28% to 53% • Metabolism • Does not inhibit P450 enzymes in vitro • Elimination
Clinical Trial • Reid IR, Miller P, Lyles K, et al. Comparison of a Single Infusion of Zoledronic Acid with Risedronate for Paget’s Disease. NEJM. 2005; 353:898-908.
Methods • Two randomized, controlled trials • independent of each other • identical protocols • Included patients from N. America, Europe, Australia, S. Africa • Pooled results in a joint analysis
Patient Selection Inclusion Criteria Exclusion Criteria Serum 25-hydroxyvitamin D level < 15ng/mL Primary hyperparathyroidism Evidence of hepatic/renal disease History of uveitis, iritis, or upper GI disorders Diabetic nephropathy/retinopathy Use of therapy specific to Paget’s disease in the preceding 180 days • Men and women > 30yo • Radiologically confirmed Paget’s disease • Alkaline phosphatase level > 2x upper limit of normal
Randomization and Treatment • Double-blind random assignment through an interactive voice-response system to receive: • A 5mg infusion of zoledronic acid over 15 minutes followed by placebo tablets for 60 daysOR • A saline infusion followed by a 30mg of risedronate per day for 60days • All patients received 1g calcium and 400-1000 U calciferol per day
Primary Study Endpoints • Proportion of patients who had a therapeutic response • Normalization of or reduction of at least 75% in alkaline phosphatase excess at 6 months • Measurements were made by Covance Central Laboratory Services
Secondary Study Endpoints • Biochemical markers of bone resorption and bone formation • QOL measured by Medical Outcomes Study 36-Item Short-Form General Health Survey (SF-36) • Bone histomorphometry • Safety assessments
Statistical Analyses • Each study had a power of 80% to demonstrate noninferiority of zoledronic acid relative to risedronate • Assumed a dropout rate of ~10% per study • Calculated would need 88 patients in each group (176 total)
Results • 182 patients enrolled in zoledronic acid group • 175 patients in the risedronate group • Similar baseline characteristics • favored male gender in the overall study population
QoL Assessment Percent of Patients with at least 5-point change at 6 months
Mean changes from baseline in the 8 domains assessed by the SF-36
Bone Biopsy • Performed in 22 patients • 12 zoledronic acid patients, 10 risedronate patients • 2 specimens (1 from each group) came from sites of Paget’s disease • Both were otherwise normal • Increased mineralization in the risedronate specimen
Adverse Events • No deaths occurred • 146 ADE in zoledronic acid group • 9 serious ADE • 133 ADE in risedronate group • 11 serious ADE • Marked clustering of ADE in first 3 days after IV drug administration • 53.7% zoledronic acid patients vs. 25.0% risedronate patients (p <0.01)
Frequencies of GI and renal or urinary disorders were similar • 1 patient in each group with preexisting renal impairment had moderate increases in SCr • Mean SCr level decreased slightly but significantly in the zoledronic acid group vs. the risedronate group by day 10 • Hypocalcemia – decreases in serum Ca++ levels in both groups at day 10
Trial Extension • Patients who met therapeutic response • Serum alkaline phosphatase measured at 6-month intervals • Median 190 days after end of core study period • 21/82 risedronate patients lost therapeutic response • 1/113 zoledronic acid patients lost therapeutic response
Weaknesses • Raw values for many statistics not reported