Download
1 / 5
50 likes | 308 Views
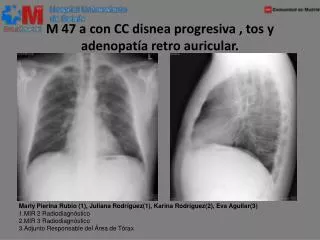
M 47 a con CC disnea progresiva , tos y adenopatía retro auricular. Marly Pierina Rubio (1), Juliana Rodríguez(1), Karina Rodríguez(2), Eva Aguilar(3) 1.MIR 2 Radiodiagnóstico 2.MIR 3 Radiodiagnóstico 3.Adjunto Responsable del Área de Tórax. TAC-AR DE TORAX. ACERCA DE ESTA ENTIDAD ….

E N D
M 47 a con CC disnea progresiva , tos y adenopatía retro auricular. Marly Pierina Rubio (1), Juliana Rodríguez(1), Karina Rodríguez(2), Eva Aguilar(3) 1.MIR 2 Radiodiagnóstico 2.MIR 3 Radiodiagnóstico 3.Adjunto Responsable del Área de Tórax
ACERCA DE ESTA ENTIDAD… 1. Identifique el hallazgo radiológico: 2.¿Cuál es el patrón característico de esta entidad? 1.Patrón en empedrado 2.Patrón quístico. 3.Engrosamiento intersticial peribronquial. 4.Nódulos centrolobulillares de distribución linfática. Rta: 4 1. Nódulos pulmonares múltiples. 2. Consolidaciones bilaterales. 3. Nódulos simétricos con mayor afectación en campos superiores y medios, adenopatías mediastínicas. 4. Patrón de “árbol en brote”. Rta: 3
SARCOIDOSIS PULMONAR Definición: enfermedad sistémica de causa desconocida, que se caracterizapor la aparición de granulomas no caseosos. Hallazgos Radiológicos: nódulos pequeños de 1- 5 mm con distribución peri linfática típicamente simétrica con mayor afectación de los campos superiores y medios asociado a aéreas de extensa fibrosis, linfadenopatias intratoracicas simétricas bilaterales. Diagnóstico: Al paciente se le realiza en diagnóstico por los hallazgos clínicos radiológico y se le realizó biopsia tras bronquial. Diagnóstico diferencial: con la beriliosis, otras neumoconiosis (silicosis y antracosis),linfangitis carcinomatosa y el linfoma. Tratamiento: Sintomático de la disnea con broncodilatadores y anti colinérgicos y corticoides que limitan la progresión del deterioro funcional.
BIBLIOGRAFIA • Nishino M, et al. A practical approach to high-resolution CT of diffuse lung disease. Eur J Radiol (2013), http://dx.doi.org/10.1016/j.ejrad.2012.12.028 • Nishino M, Lee KS, Itoh H, Hatabu H. Thespectrum of pulmonarysarcoidosis:variations of high-resolution CT findings and clues for specific diagnosis. Eur JRadiol 2010;73:66–73. • Herráez Ortega I, Alonso Orcajo N, López González L. The “sarcoidclustersign”,a new sign in high resolution chest CT. Radiologia 2009;51(5):495–9. • Nakatsu M, Hatabu H, Morikawa K, et al. Largecoalescentparenchymalnodules in pulmonarysarcoidosis: “sarcoidgalaxy” sign. Am J Roentgenol 2002;178(6):1389–93. • Kumazoe H, Matsunaga K, Nagata N, et al. Reversed halo sign” of highresolution computed tomography in pulmonary sarcoidosis. J Thorac Imaging 2009;24(1):66–8. • Webb WR, Muller NL, Naidich DP. High-resolution CT of the lung. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2000. • Traill ZC, Maskell GF, Gleeson FV. High-resolution CT findings of pulmonary sarcoidosis. Am J Roentgenol 1997;168:1557-1560. • Chiles C. Imaging features of thoracic sarcoidosis. SeminRoentgenol 2002;37:82-93.