Kaan Yücel M.D., Ph.D.
550 likes | 759 Views
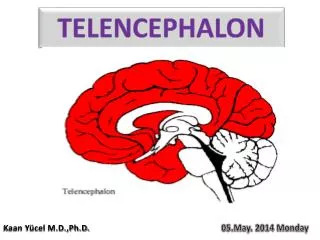
CLINICAL ANATOMY OF the LOWER LIMB. Kaan Yücel M.D., Ph.D. 15.May.2014 Thursday. CLINICAL ANATOMY OF THE LUMBOSACRAL PLEXUS. Femoral Nerve L2-L4 Largest branch of the lumbar plexus Flexors of hip & extensors of knee

Kaan Yücel M.D., Ph.D.
E N D
Presentation Transcript
CLINICAL ANATOMY OF the LOWER LIMB • Kaan Yücel M.D., Ph.D. • 15.May.2014 Thursday
CLINICAL ANATOMY OF THE LUMBOSACRAL PLEXUS
FemoralNerveL2-L4 Largestbranch of thelumbarplexus Flexorsof hip & extensors of knee Skin of theanteriorandlateralthigh, mediallegandfoot Saphenousnerve Skin of medialaspects of legandfoot Iliacus, psoasmajor, pectineus, quadricepsfemoris (rectusfemoris, vastusintermedius, vastuslateralisandvastusmedialis), sartorius ObturatorNerveL2-L4 Adductormusclesof leg Skin on thesuperiormedialthigh externaloblique, pectineus, adductorlongus, adductorbrevis, adductormagnus, andgracilis.
SciaticNerveL4-S3 • Hamstringmuscles • Extensionat thehipjoint • Flexionat thekneejoint • Commonfibularnerve • Suralcommunicatingnervelowerposterolateralside of theleg • Lateralsuralcutaneousnerveupperlateralleg • Muscles of theleg • Ant. Compartment • Dorsiflexors of ankle • Deepfibularnerve (L4, L5) • LateralCompartment • Evertors of foot & weakplantarflexors of ankle • Superficialfibularnerve(L5, S1, S2) • PosteriorCompartment • Plantarflexors of ankle • Tibialnerve (S1, S2) posteriorthighmuscles, thatflexthekneeandallmusclesthatworktheankleandfoot Tibialnerve (S1, S2) Suralnerveskin on thelowerposterolateralsurface of thelegandthelateralside of thefootandlittletoe medialcalcanealnerveskin on themedialsurfaceand sole of theheel.
FemoralNerveInjury Injuredin staborgunshotwounds, completedivision of thenerve is rare. Weaknessof hipflexion, loss of kneeextension (nopatellarreflex), sensoryloss on anteromedialthigh, knee, leg, andfoot. alongthemedialborder of thefoot as far as theball of thebigtoe; thisarea is normallysuppliedbythesaphenousnerve.
SciaticNerveInjury • Penetratingwounds • Fracturesof thepelvis • Dislocationsof thehipjoint • Mostfrequentlyinjured • during I.M. injections • Mostnervelesionsareincomplete • Commonperonealpart of thenervemostaffected • mostsuperficial in thesciaticnerve
SciaticNerveInjury Motor:Hamstringmusclesparalyzed, but weakflexion of theknee is possibletnxtosartorius(femoralnerve) & gracilis (obturatornerve). Allthemusclesbelowthekneeareparalyzed, footdrop. Sensory:Sensation is lostbelowtheknee, exceptfor a narrowareadownthemedialside of thelowerpart of thelegandalongthemedialborder of thefoot as far as theball of thebigtoe, which is suppliedbythesaphenousnerve (femoralnerve).
Sciatica [Sciaticneuralgia] Definiton:thecondition in whichpatientshavepainalongthesensorydistribution of thesciaticnerve. Symptom:Pain in theposterioraspect of thethigh, theposteriorandlateralsides of theleg, andthelateralpart of thefoot. Causes: Prolapseof an intervertebraldiscwithpressure on oneormoreroots of thelowerlumbarandsacralspinalnerves, intrapelvictumor, inflammationof thesciaticnerveorits terminal branches.
ObturatorNerveInjury Rare penetratingwounds, anteriordislocations of thehipjointabdominalherniaethroughtheobturatorforamen. pressedon bythefetalheadduringparturition. Motor:Alltheadductormusclesparalyzedexceptthehamstringpart of theadductormagnussuppliedbythesciaticnerve. Sensory:Thecutaneoussensoryloss is minimal on themedialaspect of thethigh.
ReferredPainfromtheHipJoint Thefemoralnervesuppliesthehipjoint + viaintermediateandmedialcutaneousnerves of thethigh, skin of thefrontandmedialside of thethigh. painoriginating in thehipjointto be referredtothefrontandmedialside of thethigh. Theposteriordivision of theobturatornervesuppliesboththehipandkneejoints. Thiswouldexplainwhyhipjointdiseasesometimesgivesrisetopain in thekneejoint.
PressurefromtheFetalHead on theSacralPlexus Duringthelaterstages of pregnancy, whenthefetalhead has descendedintothepelvis, themotheroftencomplains of discomfortorachingpainextendingdownone of thelowerlimbs oftenrelievedbychangingposition, such as lying on theside in bed.
Invasionof theSacralPlexusbyMalignantTumors Thenerves of thesacralplexus can becomeinvadedbymalignanttumorsextendingfromneighboringviscera. A carcinoma of therectum, forexample, can cause severe intractablepaindownthelowerlimbs.
ReferredPainfromtheObturatorNerve Theobturatornervelies on thelateralwall of thepelvisandsuppliestheparietalperitoneum. An inflamedappendixhangingdownintothepelviccavity Irritationof theobturatornerveendings Referredpaindowntheinnerside of therightthigh Inflammation of theovaries
CLINICAL ANATOMY OF THE GLUTEAL REGION
Intramuscularinjections . Theglutealregiondividedintoquadrantsbytwoimaginarylinesusingpalpablebonylandmarks linedescendsverticallyfromthehighestpoint of theiliaccrest. linehorizontalandpassesthroughthefirstlinemidwaybetweenthehighestpoint of theiliaccrestandthehorizontalplanethroughtheischialtuberosity.
GluteusMediusandMinimusandPoliomyelitis Gluteusmediusandminimus paralyzedwhenpoliomyelitisinvolvesthelowerlumbarandsacralsegments of thespinalcord. Superiorglutealnerve (L4 and 5 and S1) Problem in theability of thepatienttotiltthepelviswhenwalking.
GluteusMaximusandBursitis causedbyacuteorchronictrauma. can be extremelypainful. Thebursaeassociatedwiththegluteusmaximusarepronetoinflammation. Thegluteusmaximusbursitis is painradiatingtotheposterolateralaspect of thethigh, paraesthesiae in thelegs, andtendernessovertheiliotibialtract.
Piriformissyndrome Sciaticacausedbycompression of thesciaticnervebythepiriformismuscle Buttockpain, andlesscommonlylowbackpain, radiatinglegpainareamongthesymptoms.
Iliotibialbandsyndrome Mostcommoncause of pain on theoutside of theknee in runners, with an incidence as high as 12% of allrunning-relatedoveruseinjuries. Althoughit is not difficulttodiagnose, it can be a challengetotreat, especially in highermileagerunnerswhoplaceenormousloads on theirbodies. IliotibialBandFrictionSyndrome Injection of the anserine bursa and iliotibial tract Iliotibial Band Friction Syndrome and Greater Trochanteric Bursitis
CLINICAL ANATOMY OF THE THIGH
Ruptureof theRectusFemoris Therectusfemorismuscle can rupture in suddenviolentextensionmovements of thekneejoint. Rupture of theLigamentumPatellae This can occurwhen a suddenflexingforce is appliedtothekneejointwhenthequadricepsfemorismuscle is activelycontracting.
CollateralCirculation Ifthearterialsupplytotheleg is occluded, necrosisorgangrenewillfollowunless an adequate bypass totheobstruction is present—that is, a collateralcirculation. Suddenocclusion of thefemoralarterybyligatureorembolism, forexample, is usuallyfollowedbygangrene.
FemoralArteryCatheterization • A long, finecatheter can be insertedintothefemoralartery as it descendsthroughthefemoraltriangle. • Anatomyof Technique • Thefemoralartery is firstlocatedjustbelowtheinguinalligamentmidwaybetweenthesymphysispubisandtheanteriorsuperioriliacspine. Theneedleorcatheter is theninsertedintotheartery. • Thefollowingstructuresarepierced: • Skin • Superficialfascia • Deepfascia • Anteriorlayer of thefemoralsheath
FemoralArteryCatheterization Anatomyof Complications Enteringintothefemoralvein Piercingthepsoasmajor & enteringthehipjointcavity
Traumatic InjurytoArteries of theLowerLimb Injurytothelargefemoralartery can causerapidexsanguinationof thepatient. Unlikein theupperextremity, arterialinjuries of thelowerlimb do not have a goodprognosis. Thecollateralcirculationsaroundthehipandkneejoints, althoughpresent, are not as adequate as thataroundtheshoulderandelbow. Thefemoralartery is superficialwhere it lies in thefemoraltriangleand in consequenceeasilyinjured.
Aneurysms of theLowerExtremity MuchlessfrequentlythanabdominalaorticaneurysmsCommonsitesarethefemoralandpoplitealarteries. Patientsmaypresent in theemergencydepartmentwithcomplications, whichincludesuddenembolicobstructiontoarteriesdistaltotheaneurysmorsuddenthromboticocclusion of theaneurysm. Pressureon neighboringnervesmaygiverisetosymptoms; forexample, an enlargingpoplitealaneurysmmaypress on thetibialnerve, causingpain in thefoot.
FemoralVeinCatheterization Rapidaccessto a largevein is needed Anatomy of theProcedure 1. Theskin of thethighbelowtheinguinalligament is suppliedbythegenitofemoralnerve; thisnerveisblockedwith a localanesthetic. 2. Thefemoralpulse is palpatedmidwaybetweentheanteriorsuperioriliacspineandthesymphysispubis, andthefemoralveinliesimmediatelymedialto it. 3. At a site abouttwofingerbreadthsbelowtheinguinalligament, theneedle is insertedintothefemoralvein. Peripheral & Femoral VeinCannulation
CLINICAL ANATOMY OF THE POPLITEAL FOSSA
ArterialPalpation Arresting a severe hemorrhageorpalpatedifferentparts of thearterialtree in patientswitharterialocclusion. Femoralartery entersthethighbehindtheinguinalligament at a pointmidwaybetweentheanterosuperioriliacspineandthesymphysispubis. Poplitealartery passivelyflexingthekneejoint.
CLINICAL ANATOMY OF THE LEG
GastrocnemiusStrain Tennisleg • Painfulacuteinjuryresultingfrompartialtearing of themedialbelly of thegastrocnemius at ornearitsmusculotendinousjunction • Individualsolderthan 40 @ risk • Causedbyoverstretchingthemusclebyconcomitantfullextension of thekneeanddorsiflexion of theanklejoint
RupturedCalcanealTendon • Poorlyconditionedpeoplewith a history of calcanealtendinitis. • Audiblesnapduring a forcefulpushoff (plantarflexionwiththekneeextended) followedimmediatelybysuddencalfpainandsuddendorsiflexion of theplantarflexedfoot. • Ina completelyrupturedtendon, a gappalpable, 1-5 cm proximaltocalcanealattachment.
CalcanealTendinitis • Inflammationof thecalcanealtendonconstitutes 9-18% of runninginjuries. • Oftenoccursduringrepetitiveactivities • Especiallyin individualswhotakeuprunningafterprolongedinactivitysuddenlyincreasetheintensity of theirtraining, • Alsoresultfrompoorfootwearortrainingsurfaces.
Fabella in Gastrocnemius Close toitsproximalattachment, lateralhead of thegastrocnemiuscontains a sesamoidbone Fabella(L. bean) Articulateswiththelateralfemoralcondyle Visiblein lateralradiographs of theknee in 3-5% of people
SuperficialFibularNerveEntrapment Chronicanklesprainsmayproducerecurrentstretching of thesuperficialfibularnerve Pain alongthelateralside of thelegandthedorsum of theankleandfoot. Numbnessandparesthesia (ticklingortingling)
DeepFibularNerveEntrapment Excessiveuse of musclessuppliedbythedeepfibularnerve (e.g., duringskiing, running, anddancing) mayresult in muscleinjuryandedema in theanteriorcompartment. Compressionof thedeepfibularnerveandpain in theanteriorcompartment. Painoccurs in thedorsum of thefootandusuallyradiatestothe web spacebetweenthe 1st and 2nd toes.
InjurytoCommonFibularNerve& Footdrop • Superficialcoursearoundfibularneck • Mostinjurednerve in thelowerlimb • Flaccidparalysis of allmuscles in theanteriorandlateralcompartments of theleg • dorsiflexorsof ankleandevertors of foot • Lossof dorsiflexion of theankle • footdrop • furtherexacerbatedbyunopposedinversion of thefoot
InjurytoCommonFibularNerve& Footdrop • Becausethedroppedfootmakes it difficulttomaketheheelstrikethegroundfirst as in a normal gait, steppagegait • Sometimesan extra “kick” is added as thefreelimbswingsforward in an attempttofliptheforefootupwardjustbeforesettingthefootdown.
Injurytotibialnerve Motor: Allthemuscles in theback of thelegandthe sole of thefootareparalyzed. Theopposingmusclesdorsiflexthefootat theanklejointandevertthefootat thesubtalarandtransversetarsaljoints, an attitudereferredto as calcaneovalgus. Sensory: Sensation is lost on the sole of thefoot; later, trophiculcersdevelop.
PosteriorTibialPulse Between posteriorsurface of medialmalleolus & medialborder of calcanealtendon Posteriortibialartery passesdeeptoflexorretinaculum Whenpalpatinghavetheperson invertfoottorelaxtheretinaculum Absenceof posteriortibialpulses Signof occlusiveperipheralarterialdisease in peopleolderthan 60 years Intermittentclaudicationcharacterizedbylegpainandcramps, duringwalking
VaricoseVeins • A varicosedvein • Largerdiameterthannormal, elongated & tortuous • Commonlyoccurs in thesuperficialveins of thelowerlimb • Responsibleforconsiderablediscomfortandpain • Every time thepatientexercises, high-pressurevenousbloodescapesfromthedeepveinsintothesuperficialveinsandproduces a varicosity, andgetsworseby time.
DeepVeinThrombosis& Long-DistanceAir Travel • Passengerswho sit immobileforhours on long-distanceflightsareverypronetodeepveinthrombosis in thelegs. • Preventativemeasuresincludestretching of thelegseveryhourtoimprovethevenouscirculation. Prevention of deep vein thrombosis associated with flying ArchInternMed. 2003;163:2766-2770. Incidence of airtravel-relatedpulmonaryembolism at the Madrid-Barajasairport. Pérez-Rodríguez E, Jiménez D, Díaz G, Pérez-Walton I, Luque M, Guillén C, Mañas E, Yusen RD.
Popliteal, Anterior, & PosteriorTibialArteries Poplitealarteryocclusionjustbelowthebeginning of theartery justbelowtheopening in theadductormagnusmuscle Insomecasesextendsdistally originsof theanterior& posteriortibialarteries,evenperonealartery. intermittentclaudication, nightcramps, and rest paincausedbyischemicneuritis. trophicchanges impairedorabsentarterialpulses, lowered skin temperature, colorchanges, muscleweakness, andtrophicchanges
CLINICAL ANATOMY OF THE FOOT
Morton'sneuroma • Enlargedcommonplantarnerve • @ thirdinterspace • betweenthird &fourthtoes • 3rd interspace, lateralplantarnerveoftenuniteswithmedialplantarnerve. • "Pushoff" phase of walkinginterdigitalnervesandwiched • betweenground & deeptransversemetatarsalligamentabove • Compressingcommonplantarnerve • Painin thethirdinterspace
Tarsaltunnelsyndrome Posteriortibialneuralgia • Compressionneuropathy& a painfulfootconditionwheretibialnerve is compressedthroughthetarsaltunnel • Numbnessin thefoot, radiatingtothebigtoeandthefirst 3 toes, pain, burning, electricalsensations, andtinglingoverthebase of thefootandtheheel.
PlantarFasciitis • Occursin individualswho do a greatdeal of standingorwalking, painandtenderness of the sole of thefoot. • Believedto be causedbyrepeatedminortrauma. • Repeatedattacks of thisconditioninduceossification in theposteriorattachment of theaponeurosis, forming a calcanealspur.
ClinicalProblemsAssociatedWithArchesof theFoot • Mediallongitudinalarch • largest &clinicallythemostimportant • Intheactivefootthetone of muscles • an importantfactor in archsupport. • Musclesarefatigued • excessiveexercise • standingforlongperiods • overweight • illness • muscularsupportgivesway, theligamentsarestretched, andpain is produced.
Pes planus(Flatfoot) • Mediallongitudinalarch is depressedorcollapsed. • Forefootis displacedlaterallyandeverted. • Themusclesandtendonsarepermanentlystretched. • Congenital & acquired