Download

1 / 76
770 likes | 913 Views
PARTNER – at Pavia, January 2012 LET and Fractionation. Bleddyn Jones University of Oxford Gray Institute for Radiation Oncology & Biology 21 Century School Particle Therapy Cancer Research Institute, Oxford Physics. LH Gray

E N D
PARTNER – at Pavia, January 2012 LET and Fractionation Bleddyn Jones University of Oxford Gray Institute for Radiation Oncology & Biology 21 Century School Particle Therapy Cancer Research Institute, Oxford Physics.
LH Gray • studied neutron effects in biological systems. • thought that neutrons were a good tool for research, but not suitable for cancer therapy. • was opposed by a medical doctor, Constance Wood. • She dismissed Gray from the post of Director of Physics at Hammersmith Hospital. • Dr Wood had used her family fortune (from brewing beer) to develop first European clinical linear accelerator, produced by the Vickers Company (who built aeroplanes, submarines, radar equipment etc.)
From Fowler, Adams and Denekamp : Cancer Treat. Reviews 1976, 3, 227-256
‘Megamouseexpt’ at Northwood Gray Lab, Fowler, Sheldon, Denekamp, Field (IJROBP, 1, 579-92, 1976) Deterioration due to repopulation % Tumour control for same level of skin reaction in mice Improvement at short times with metronidazole or neutrons (compensating for hypoxia) Improvement due to cell cycle progression, reoxygenation Overall time in days (also related to number of fractions)
Adding a repopulation correction factor to LQ model So, fractional increase in number of cells is obtained from equation 1 and 2 • Surviving fraction describes a reduction in viable cell numbers but is opposed by repopulation • If there are c cells at start of radiation there will be c.SF after radiation. • The clonal expansion during radiotherapy is represented by Nt=Noe-kg.t, [eq 1] where t is the elapsed time when No cells become Nt cells and kg is the growth rate constant • When Nt/No=2 the population will have doubled, so that the time is then the doubling time of cells……..that is 2=e-kgTp…….so that ln2=-kKg.Tp [eq 2] and so kg can be replaced by ln2/Tp in eq 1 above Let this ratio be the repopulation correction factor (RCF) as it opposes cell kill; Net number of cells after treatment over a time t becomes = c. SF x RCF
Full LQ equation with allowance for repopulation The net surviving fraction is This is a powerful equation with many applications ….the lowest surviving fraction will be obtained with highest dose and highest radiosensitivities and longest doubling times and shortest overall time See Fowler 1988 Progress in Fractionated Radiotherapy, Brit J Radiology Fowler showed that different fractionation schedules could have similar tumour control rates when overall time and repopulation included .
Some general principles • As f(inter-fraction interval) reduces • time to repair radiation damage…more incomplete repair present at next treatment …enhanced effects in late reacting normal tissues • opportunity for tumour cell repopulation As n increases More opportunities for repair between fractions T then increases unless f is reduced in which case treatment is accelerated As T increases…more time for • normal tissue repair and repopulation…less severe acute reactions • tumour repopulation, so cure rate may fall if fast cellular doubling times • Re-oxygenation of hypoxic tumours If d increases, D(=n.d) must be reduced to preserve iso-effect/ tissue tolerance
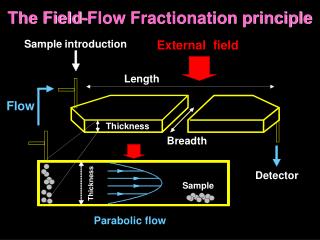
Ionising Radiation and DNA+ microdosimetric theories Densely ionising radiation (high-LET) e.g. -particles C6+ ions High concentration of ionisation events Sparsely ionising radiation (low-LET) e.g. -rays, -particles Low concentration of ionisation events electron tracks Dr Mark Hill, Gray Institute, Oxford DNA
RBE depends on …….. Particle,Energy & Depth Target Volume Dose per treatment ..RBE varies inversely with dose. A treatment plan contains many dose levels. Facility: neutron & -ray contamination Cell & Tissue type : slow growing cells have highest RBEs. Use of single value RBE was mistake
Paravertebral Epithelioid SarcomaIntensity Modulated Protons (IMPT) vs. Intensity Modulated Photons (IMRT) 7 (field) IMPT IMXT
Esophageal radiotherapy dose distributions – Protons vs. IMRT
Track structure on the nuclear/cellular scale H2AX H2AX -particle Chromosome domains High-LET (e.g. -particles) Low-LET (e.g. -rays) 1 Gy corresponds to: ~2 alpha tracks ~1000 electron tracks ~20-40 DSB (~20% complex) 1 lethal chromosome break ~20-40 DSB (~70% complex) 3 lethal chromosome breaks Relatively homogeneous Very non-homogeneous
Biological effects More cell kill per unit dose. Enhanced Biological effects Need single dose RBE (x-ray dose/neutron dose for equal bio-effect ) to estimate required neutron dose to give same effect as x-rays or -ray Cobalt beam.
RBE – components in a ratio Changes with dose per fraction and cell cycling in repair proficient cells Little or no changes in required dose with dose per fraction and cell cycling in repair proficient cells; but this dose follows the numerator and reduces sharply because of tending to Rmax
Reduced repair capacity at high LET α parameter increases by more than the increase in β [ e.g. 2.5-3 compared with 1.3 for fast neutrons] Then, α/β increases with LET and so “fractionation sensitivity” reduces α –related damage is less repairable than β related damage.
X-rays Radioresistant cells with greatest curvature (higher DNA repair capacity) show higher RBEs (GSI, Weyreuther et al) RBE depends on Cell Type and its / ratio which reflects repair capacity Carbon ions
Recovery ratio – the ratio of surviving fractions for one and two fractions to same total dose. For low LET radiations
So, the capacity for repair with standard x-rays is higher by a factor of: For iso-effect Now RBE>1 and RBE>Rmin, dH>1 So RR of low LET radiation always exceeds that of high LET
Another method Consider the change in the number of fractions N for the same effect when dose per fraction is changed; assume N is continuous variable. Where α/β=k Numerator term in parentheses is smaller than denominator squared term in parentheses for increasing Rmax and Rmin compared with unity for low LET [for equal k, d and BED]
LOW LET change in total dose with number of fractions (or dose per fraction)
LOW LET: change in total dose with number of fractions (or dose per fraction)
The medical prescription Cobalt Gray equivalent (coGyeq) or X-ray equivalent Gray (eqGy) Intended dose (i.e. x-ray dose) is divided by the RBE (relative biological effect). Traditionally, RBE is a constant factor, e.g. 3 for neutrons, 1.1 for protons, 2.5 for C ions….to all tissues & at all doses in body….and - independent of α/β ratio 45 Gy in 15# 45/3=15 coGyeq neutrons Experiments: assumption not true for neutrons (& C ions), but what about protons?
Neutron TherapyPrescription of radiation using fixed RBE of 3 at tumour depth and assumed to be the case at all other points within a patient (all tissues, all doses). The pseudo exponential dose fall-off with depth beyond a tumour will be compensated for by increase in RBE. RBE=2.5 RBE=4-6 RBE=3 Using more fields will only make matters worse
BED - how do we get there? By definition of the “Log cell kill”=E
BED - The Concept • Represents total dose if given in smallest fraction size
How can we picture BED for high LET radiations? Dose for same effect in four fractions Dose for same effect in single fraction DOSE (Gy) BED Surviving Fraction All have same Effect/ Single fraction Imagine the dose to be given in infinitely small fractions with no curvature to slope High LET shifts all curves to left, but effect defined by same low LET BED
BED - some implications Any two schedules can either be compared or equated An exact solution can only be obtained for a specific / value Solving for d when / changes will give a different answer BED values must be qualified by the / ratio used
Fowler`s ‘FE’ – fractionation effect plot • E=n(d+d2) • E=D(+d) • Divide throughout by E and by D, so /=intercept/slope 1/D tan=/E /E y = c + mx d = - /
Use of BED • Refers to points/small volumes of interest; can be extended to volumes as in EUD. • Comparisons are for individuals • Iso-effect calculations, ranking of BEDs for comparisons of different techniques/schedules. • Compensation for errors in dose delivery and unscheduled treatment extensions • Dose rate effects • Generic comparisons of different fractionation schedules in radiotherapy – including high and low LET radiations Reference: Jones B, Dale RG, Deehan C, Hopkins KI, Morgan DAL. The role of biologically effective dose (BED) in Clinical Oncology. Clinical Oncology 2001;13:71-81. Jones B and Dale RG. Radiobiological compensation of treatment errors in radiotherapy. Brit J Radiology, 81, 323-326, 2008. Dale RG, Hendry JH, Jones B, Deehan C et al. Practical methods for compensating for missed treatment days in radiotherapy, with particular reference to head & neck schedules. Clinical Oncology, 14, 382-393, 2002.
The fractionated isoeffect equation • Obtaining BED: • Divide throughout by αL to give BED on LHS. • It follows that RHS, also divided by αL, represents the for the high LET radiation. • Note if NL=NH, roots are simpler, and RBE is then the ratio of doses per fraction.
Useful equations for high LET radiations RBE is defined as dL/dH = the RBE at low dose = the RBE at high dose The RBE between RBEmax and RBEmin is given by solving the first equation for dL, and then divide by dH, so that Where k is the low LET / ratio Jones, Carabe and Dale BJR 2006 – adapted for treatment interruption calculations
Biological Effective Doses for High LET radiation • the low LET / ratio is used • RBEs act as multipliers of the low LET α/β • RBE values will be between RBEmax and RBEmin depending on the precise dose per fraction • KL is daily low LET BED required to compensate for repopulation KH/RBEmax
Note: • RBEmax is intercept on y axis, • RBEmin is asymptote at high dose • A fixed RBE, of say 3, would intersect all curves
Applications Converting a specific low LET BED to that for high LET, when the low LET α/β ratio is known……use
For isoeffect calculations in the case of two high LET schedules – need (α/β)H value . And so, = where Then, for N1H(αHd1H+βHd1H2)= N2H(αHd2H+βHd2H2) Divide throughout by αH = - KHT1H= - KHT2H
Some important caveats – slide 1 • Use same α/β ratio across isoeffect equations to preserve units • Changing fractionation numbers between low and high LET radiation introduces a complication. RBE should be specific for the dose per fraction used.
Some important caveats – slide 2 • If fraction numbers differ, work out equivalent low LET dose/# for same # Number as the proposed high LET schedule and then convert, or use the equations with RBEmax and RBEmin and fraction numbers (NL and NH). • Beware of “fractionated RBEs” based on total doses when NLNH (suggested by Dasu & Dasu) – Suggest always use single dose RBE and then compensate for fractionation
Question: Estimate the dose/# required for a 10 fraction high LET schedule equivalent to 30# of 2 Gy [low LET] for CNS tissue α/β=2 Gy for RBEmax=6 and RBEmin=1.25. First, find equivalent of 30# schedule in 10 #:- 30(1+2/2)=10dL(1+dL/2); dL=4 Gy Then find dH in: 10*dH(6+1.252*dH/2) =10*4 (1+4/2) dH=1.69 Gy. Note the RBE per fraction is then 4/1.69=2.37 Alternatively we could calculate dH direct from 10*dH(6+1.252*dH/2) =30(1+2/2) dH=1.69 Gy. But the RBE is not 2/1.69=1.18 Use RBE on dose per fraction basis for equal No of #.
Q2: A tumour boost of 3 Gy-eq dose per fraction for 6 fractions delivers, incorrectly, 4 Gy-eq for the first two fractions. What dose should be given in the remaining fractions to maintain same tumour control (assuming α/β=9 Gy and late CNS isoeffect α/β=2 Gy, and RBE of 3 for the Gy-eq calculation. For CNS, intended low LET BED = 6*3(1+3/2) =45 Gy2. Delivered BED=2*4(1+4/2)=24 Gy2. Deficit = 45-24=21 Gy2 In 4 remaining fractions, need 4*d(1+d/2)=21; d= 2.39 Gy-eq. [or 2.39/3= 0.8 Gy high LET] For tumour control, solve same steps for α/β=9 Gy , giving d=2.45 Gy-eq; a higher dose. So, to maintain same tumour control need to exceed CNS BED…..!
BUT …Previous slide presumes RBE does not vary with dose per fraction! If the actual doses of high LET given were intended: 3/3=1 Gy/# and in first two fractions was actually 4/3=1.33 Gy/# Then, if RBEmax=6, RBEmin=1.25 in CNS Intended BED=6*1 (6+1*1.252/2)=40.69 Gy2. Delivered BED= 2*1.33(6+1.33*1.252/2)=18.17 Gy2 Deficit BED= 40.69-18.17=22.52 Gy2 The dose, dH, then required in remaining 4 # is found by solving: 4 dH(6+dH*1.252/2)=22.52 dH=0.86 Gy of high LET; NOTE this is a different result to the previous page [dH=0.8 Gy] due to RBE changing with dose per# …..WE MUST IMPROVE SYSTEM!
Worked example of a time delay Schedule: megavoltage X-ray of 45 Gy in 25 fractions, then ‘boost’ of 6 Gy[physical dose] in 2 fractions using a high-LET radiation with RBEmin= 1.3 and RBEmax =8. There is a delay of one week in delivery of boost, due to patient illness. Assume tumour daily repopulation equivalent of 0.6 Gy per day after a lag interval of 25 days during megavoltage x-ray treatment; normal tissue / =2 Gy, tumour / = 10 Gy.
Worked example -II • The intended BED to normal tissue from x-rays = 45 (1+1.8/2)= 85.5 Gy2 • The intended BED to any marginal normal tissue that receives the added high-LET boost of 2 fractions of 3 Gy = 6 (8+1.323/2)= 63.2 Gy2 • total intended maximum BED to same volume of normal tissue = 85.5 + 63.2 = 148.7Gy2
Worked example -III • The intended BED to tumour by x-rays = 45 (1+1.8/10)=53.1 Gy10 • the intended BED to tumour by high LET = 6 (8+1.32 3/10)=51.04 Gy10 • So, total tumour BED is 53.1+52.04=104.14 Gy10 before allowing for repopulation • The additional seven days of repopulation must be allowed for because of the treatment interruption in providing the boost, which is equivalent to 0.6 7=4.2 Gy10.
Worked example - IV • The boost must accommodate the original high-LET BED plus 4.2 Gy, i.e. 51.04 + 4.2 = 55.24 Gy10 • As this is to be given in two fractions, then : 2d (8+1.32d/10)=55.24, d = 3.23 Gy/fraction - instead of the original 3 Gy per fraction. BUT Normal tissue BED is : 23.23(8+1.323.23/2) = 69.31Gy2. • Total (low plus high-LET) normal tissue BED increases by 69.31 - 63.2 = 6.11Gy2, ( 4.1% increase) in order to maintain the same tumour BED. This might increase tissue side effects. • A compromise solution e.g. 3.15 Gy instead of 3.23 Gy might be used. This would lead to 67.17 Gy2 maximum high-LET BED to the normal tissues and 53.75 Gy10 to the tumour.
Summary : • RBE is likely to be related to low LET(control) α/β ratio in two ways : • Inversely at lower doses where RBEmax dominates • Directly at high doses where RBEmin dominates
From previous definitions of RBEmax and RBEmin Then impose boundary conditions on lower limit of each RBE ( the RBE due to change in beam physics alone)
L=Low LET, H=High LET RBEMAX = αH/αL RBEMIN =(βH/βL) RBEMAX = A+B/(α/β)L RBEMIN = C+K(α/β)L Fast neutron data Hammersmith and Clatterbridge data. Then replace the two RBE limits in: BED[highLET] =DH(RMAX+RMIN2dH/(α/β)L) BED[lowLET] =DL(1+dL /(α/β)L)
We can then replace RBEmax and RBEmin with functions of α/β in And then solve roots to obtain ‘flexible’ RBE as:
Four examples from Hammersmith animal neutron experiments – (Carabe-Fernandez et al IJRB 2007) Kidney Oesophagus..acute RBE SKIN Lung RBE