Download
1 / 1
10 likes | 111 Views
Prolonged Recovery from Succinylcholine Necessitating Mechanical Ventilatory Support in a Pregnant Patient Gregory Kozlov DO and David J. Lang DO Department of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL 60657 USA. Abstract. Discussion.

E N D
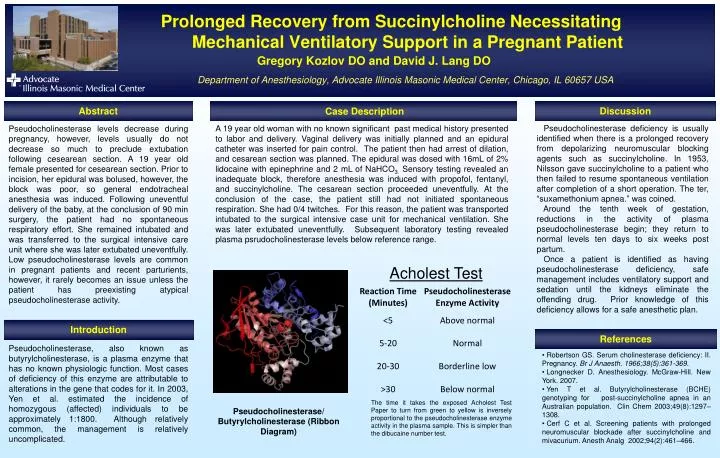
Prolonged Recovery from Succinylcholine Necessitating Mechanical Ventilatory Support in a Pregnant PatientGregory Kozlov DO and David J. Lang DO Department of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL 60657 USA Abstract Discussion Case Description Pseudocholinesterase deficiency is usually identified when there is a prolonged recovery from depolarizing neuromuscular blocking agents such as succinylcholine. In 1953, Nilsson gave succinylcholine to a patient who then failed to resume spontaneous ventilation after completion of a short operation. The ter, “suxamethonium apnea.” was coined. Around the tenth week of gestation, reductions in the activity of plasma pseudocholinesterase begin; they return to normal levels ten days to six weeks post partum. Once a patient is identified as having pseudocholinesterase deficiency, safe management includes ventilatory support and sedation until the kidneys eliminate the offending drug. Prior knowledge of this deficiency allows for a safe anesthetic plan. A 19 year old woman with no known significant past medical history presented to labor and delivery. Vaginal delivery was initially planned and an epidural catheter was inserted for pain control. The patient then had arrest of dilation, and cesarean section was planned. The epidural was dosed with 16mL of 2% lidocaine with epinephrine and 2 mL of NaHCO3. Sensory testing revealed an inadequate block, therefore anesthesia was induced with propofol, fentanyl, and succinylcholine. The cesarean section proceeded uneventfully. At the conclusion of the case, the patient still had not initiated spontaneous respiration. She had 0/4 twitches. For this reason, the patient was transported intubated to the surgical intensive case unit for mechanical ventilation. She was later extubated uneventfully. Subsequent laboratory testing revealed plasma psrudocholinesterase levels below reference range. Pseudocholinesterase levels decrease during pregnancy, however, levels usually do not decrease so much to preclude extubation following cesearean section. A 19 year old female presented for cesearean section. Prior to incision, her epidural was bolused, however, the block was poor, so general endotracheal anesthesia was induced. Following uneventful delivery of the baby, at the conclusion of 90 min surgery, the patient had no spontaneous respiratory effort. She remained intubated and was transferred to the surgical intensive care unit where she was later extubated uneventfully. Low pseudocholinesterase levels are common in pregnant patients and recent parturients, however, it rarely becomes an issue unless the patient has preexisting atypical pseudocholinesterase activity. Introduction References Pseudocholinesterase, also known as butyrylcholinesterase, is a plasma enzyme that has no known physiologic function. Most cases of deficiency of this enzyme are attributable to alterations in the gene that codes for it. In 2003, Yen et al. estimated the incidence of homozygous (affected) individuals to be approximately 1:1800. Although relatively common, the management is relatively uncomplicated. • Robertson GS. Serum cholinesterase deficiency: II. Pregnancy. Br J Anaesth. 1966;38(5):361-369. • Longnecker D. Anesthesiology. McGraw-Hill. New York. 2007. • Yen T et al. Butyrylcholinesterase (BCHE) genotyping for post-succinylcholine apnea in an Australian population. Clin Chem 2003;49(8):1297–1308. • Cerf C et al. Screening patients with prolonged neuromuscular blockade after succinylcholine and mivacurium. Anesth Analg 2002;94(2):461–466. The time it takes the exposed Acholest Test Paper to turn from green to yellow is inversely proportional to the pseudocholinesterase enzyme activity in the plasma sample. This is simpler than the dibucaine number test. Pseudocholinesterase/ Butyrylcholinesterase (Ribbon Diagram)






