Download
1 / 37
370 likes | 534 Views
Cost Benefit Analysis of Influenza Vaccination of Healthy Adults. Influenza in the Workplace / Health Care Setting. Morbidity with Influenza in Adults. Singh S. Clin Drug Invest 2003; 23: 561. Mean Duration of Symptoms in University Students with Colds & ILIs. All P values < .001.

E N D
Cost Benefit Analysis of Influenza Vaccination of Healthy Adults
Morbidity with Influenza in Adults Singh S. Clin Drug Invest 2003; 23: 561.
Mean Duration of Symptoms in University Students with Colds & ILIs All P values < .001
Time to Afebrile State in Adults with Influenza Singh. Clin Drug Invest 2003; 23: 561.
QALDs for Healthy Adults with Influenza Turner. Health Technol Assess. 2003: 7(35): 122.
ILI Among Adults, 2004 MMWR 2004; 53: 1156-8.
Some Complications are Common in Low Risk Groups [1] Belshe RB et al. Pediatr Infect Dis J 2000; 19: S66. [2] Kaiser L, et al. Arch Intern Med 2000; 160: 3234. [3] Kaiser L, et al. Arch Intern Med 2003; 163: 1667.
Influenza Virus Infection in Travelers to Tropical & Subtropical Countries • 1450 Swiss travelers (1998-2000) • 19.9% had febrile illness during / after travel • 12.8% had seroconversion to influenza • 2.8% of all travelers had seroconversion (incidence of 1% per travel-month) • 62.5% acquired influenza outside of European flu season Mutsch M et al. CID 2005; 40: 1282-7.
Overview • Definitions • CBA of healthy working adults study • Context • Challenges
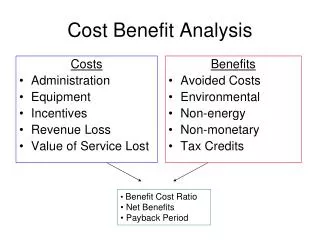
Definitions • Cost Effectiveness Analysis (CEA) • Cost per health outcome (eg $ per life saved) • Cost Utility Analysis (CUA) • Cost per unit of quality adjusted health outcome (eg $ per quality adjusted life year [QALY]) • QALY incorporates impact on both quantity & quality of life • Cost Benefit Analysis (CBA) • All outcomes assigned a dollar value; results presented as net costs or savings.
Economic Analysis Metrics • CEA • ratio ($ / outcome) • CUA • ratio ($ / QALY) • CBA • Net $
Monetary Cost Equation (numerator) Intervention Costs - Costs Averted Net Costs (Savings) * Net costs (savings) become the numerator for CEA & CUA ratios. Represent net value for CBA. * Different monetary costs may be included in different types of analyses.
Types of Monetary Costs Typically Included • CEA denotes cost effectiveness analysis. • CUA denotes cost utility analysis. • CBA denotes cost benefit analysis.
Caveats • Cost effective cost saving • Cost saving interventions are dominant • “Cost effective” interventions can be considered for adoption • They don’t need to be cost saving to be worthwhile • Depends on the “cost effective” threshold • Also depends on importance of disease, feasibility, etc • Cost saving “must do” • CEA CUA CBA (they are different metrics)
Cost-Benefit Analysis of a Strategy to Vaccinate Healthy Working Adults Against Influenza Arch Intern Med 2001; 161: 749-59
CBA Model • Societal perspective • Nationally representative estimates • Accommodated year-to-year variability of influenza & vaccine effectiveness • Incorporated plausible ranges / variation in other clinical & cost variables • Conservative base case values • Sources of data = published literature, many studies, many seasons
Approach to Costs * Vaccine & administration • Assumed delivery in low cost / efficient settings • Productivity costs • Human capital approach • Hospitalization costs • Charges adjusted by Medicare cost-to-charge ratio • Time preference (ie discounting) included • All costs adjusted to appropriate year using CPI
Analysis • Monte Carlo simulation • Probability distributions for uncertain variables • Multivariate regression modeling • Sensitivity analyses
Mean Costs per Person Vaccinated Total $16.69 Total $30.34
Mean Costs by Type of Cost Net Savings = $13.66 per person vaccinated
Validation of Selected Model Outcomes From Clinical Trial Data Reduction with Vaccination (no. per 100 persons vaccinated) • Nichol KL. Arch Intern Med 2001; 161: 749. • Nichol KL, et al. Vaccine 2003; 21: 2216. • Demicheli V. Cochrane Database of Systematic Reviews 2004 (3).
Challenges from the literature • Cochrane review of influenza vaccination for healthy adults, 2004 • Results • VE lab confirmed flu 70% (56% - 80%) • VE clinical ILI 25% (13% - 35%) • ARR 6% • Work loss decreased by .16 days (.04 - .29) • Conclusions: Influenza vaccines are effective in reducing serologically confirmed influenza. However they are not as effective in reducing cases of clinical influenza & number of working days lost. Universal immunization of healthy adults is not supported by the results of this review.
Outcome / case definition & RRR vs ARR • Typical kinds of outcomes assessed in VE studies • Cause specific (specific outcomes) • Infection • Lab confirmed illness (LC ILI) • LC Influenza + otitis media • “All cause” (sensitive outcomes) • Clinical illness (ILI) without lab confirmation • Complications • Otitis media • Pneumonia hospitalization • Death • Cause specific outcomes provide highest RRR because there is less “noise” • But this does not mean that the lower RRR seen with all cause outcomes means that the vaccine is less effective (ie the ARR would be the same or greater if it could be measured)
Summary • Vaccination of healthy younger adults reduces illness, provider visits and work loss • Vaccination is also likely to provide economic benefits
US Economic Studies of Influenza Vaccination in Working Adults 1. NEJM 1995; 333: 889. 2. JAMA 2000; 284: 1655. 3. Vaccine 2003; 21: 2216. 4. JAMA 1983; 249: 3189. 5. Emerg Infect Dis 1999; 5: 659. 6. Arch Intern Med 2001; 161: 749 7. Clin Infect Dis 2001; 33: 1879. 8. Ann Intern Med 2002; 137: 225. 9. Am J Med 2005; 118: 68.
CEA Studies of Influenza Vaccination of Working Adults Around the Globe 1. Nichol KL. Vaccine 2003; 21: 1769; 2. Turner D et al. HTA 2003; 7(35). 3. Martin DJ. Occup Health SA 1997; 3: 23; 4. Rothberg MB. Am J Med 2005; 118: 68. 5. Postma MJ. Vaccine 2005.
Median Cost-Utility Ratios for Selected Clinical Preventive Services Stone PW, et al. Am J Prev Med 2000; 19: 15 – 23.
Context: Cost Effectiveness of Selected Childhood Immunizations
Outstanding Issues / Knowledge Gaps • Appropriate application and interpretation of data • Threshold for defining “cost effective” • Epidemiology of disease, complication rates, health care use, & impact on productivity • Over time & by region • Productivity measures • Impact of reduced work effectiveness • Attenuation of illness • Caregiver time • Secondary cases • Costs & benefits of vaccination by setting and compliance level & implications of herd immunity • Feasibility & vaccine supply
Impact of More Sensitive Outcomes on ARRMore sensitive outcomes will have a higher ARR – ie they are more inclusive Nichol KL. Virus Res 2004; 103: 3 – 8.