
Uploaded by
anila
0 SLIDES
179 VIEWS
0LIKES
Moral Hazard
DESCRIPTION
Moral Hazard. Hospitals. Outline. Evolution of the Modern Hospital Economic Rational for the Non-Profit Hospital How Do Hospitals Compete? Provider Consolidation Hospital Pricing. Evolution of the Modern Hospital.
Download

1 / 0
Download Presentation 
Moral Hazard
An Image/Link below is provided (as is) to download presentation
Download Policy: Content on the Website is provided to you AS IS for your information and personal use and may not be sold / licensed / shared on other websites without getting consent from its author.
Content is provided to you AS IS for your information and personal use only.
Download presentation by click this link.
While downloading, if for some reason you are not able to download a presentation, the publisher may have deleted the file from their server.
During download, if you can't get a presentation, the file might be deleted by the publisher.
E N D
Presentation Transcript
- Moral Hazard
-
Hospitals
- Outline Evolution of the Modern Hospital Economic Rational for the Non-Profit Hospital How Do Hospitals Compete? Provider Consolidation Hospital Pricing
- Evolution of the Modern Hospital Most hospitals in the late 19th and early 20th century functioned as almshouses and pesthouses. Places for the poor Funded by private charity Those who had money could afford to die at home. As medical science advanced the hospital came to the center of medical care
- The History of U.S. Hospitals Hill Burton Act of 1946 provided funding to refurbish old hospitals and to build new hospitals The increased prevalence of health insurance in the 1950s resulted in an increase in demand for hospital services Creation of Medicare & Medicaid increased demand Period of downsizing Introduction of Prospective Payment Systems Growth of managed care
- Hospitals by Type By Year
- Hospital Beds by Type By Year(in 1000s)
- Hospital Occupancy
- Hospital Trends Hospital ALOS on the decline PPS encouraging “quicker and sicker” discharges Managed care limiting hospital stays Growth of alternative services Movement to outpatient settings 84% of U.S. community hospitals have less than 300 beds Rural hospitals average 65 beds; urban hospitals 231 5.7 million hospital employees (40% of health care workforce, 4% of employed civilians) Current trend is to downsize employment Average hourly earnings highest among healthcare sites
- Evolution of the Hospital Downward trend in the number of hospitals Expected to continue as consolidation continues and care moves out of the hospital. For-profit hospitals are on the rise, but Nonprofits are still a large majority, why?
- The Nonprofit Hospital Contract failure Asymmetric information Shopping problem Trust between patient and physician Public goods Inertia Many “nonprofits” make a large profit Tax exempt vs nontax exempt
- What is the Objective a Non-Profit Hospital? Most firms exist to maximize profits But for a NFP, what is their objective? “Profit” Maximization No Margin, no mission? Utility Maximization Physician Control
- How do For Profit Hospitals Compare to Private Non Profits? Costs and Pricing Uncompensated Care 4.5% vs 4% Quality Entry and Exit NFP quicker to enter a new market and slower to exit Bottom Line: Very hard to “see” a difference
- Hospital FinancingPayment-to-cost ratio
- How do Hospitals Compete? Normally competition leads to lower prices and decreased costs. In hospitals it is often argued the opposite occurs. Some research shows that when hospital markets become more competitive there is increased costs and higher prices to consumers Policy implications are to discourage competition
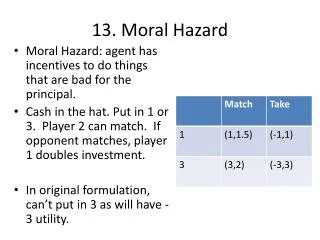
- The decision to specialize Hospital 1 Basic only Both $5,000 $10,000 Basic Only $5,000 $2,000 Hospital 2 $2,000 $3,000 Both $10,000 $3,000
- Hospital Competition Medical Arms Race “Consumer-Driven” Competition Hospitals compete not in the price/quality space but in a “relative” competition Physicians Perceived quality relative to competitors Incentive to over-invest in technology and expand into “unprofitable” services
- Hospital Competition Policy Reaction to MAR CON Laws Hospitals must justify the need is there for a particular service or facility prior to adding it. Non CON states such as Texas have seen some of the largest examples of this type of behavior Anti-Trust Policy Implication is that monopolies are not so bad Mergers that would have been blocked in other industries have been allowed in hospitals
- Hospital Competition Evidence on MAR Research prior to the 1990s tends to find that when markets become more competitive, then there is an increase in costs and consumers face higher prices. Contrary to standard economic theory Research looking at data in the 1990s found the opposite: More competitive markets resulted in lower prices and costs
- Hospital Competition Payer Driven Competition When hospitals compete for patients via insurance contracts, we find markets tend to work well. In most markets the individual paying the bill and consuming the product are the same so this is not an issue Selective contracting By the end of the 1990s the Medical Arms Race was considered dead But as consumers have demanded choice in providers, selective contracting has become much less selective Robotic Surgery Proton Beam Therapy Children’s hospitals Policy should be focused on getting providers to compete for contracts.
- Provider Consolidation Consolidation Trend in the 1990s
- Rise of Local Hospital Systems
- A New Wave?
- Merger and Acquisition The Affordable Care Act represented a "tectonic shift" in the way hospitals do business and many are left with few choices but to be acquired or merge with another entity.
- It is not just acquisition Affiliation Most flexible form of consolidation Utilized to increase footprint, gain economy of scale, create referrals, etc Do not necessarily change management or governance Joint Venture Mildly flexible Used to create something new that might be overwhelming to do solo Shared governance Some for of profit/risk sharing
- It is not just acquisition Joint Operating Agreement Virtual mergers – assets may separate but services are coordinated New overarching governance board, but hospitals maintain independent boards as well May borrow for capital investments as one organization Similar to JV but larger
- It is not just acquisition Merger Mutual decision of two companies to combine Leadership may be a combination of the two hospitals or from an outside source Hospitals absorb each other’s assets and debts Acquisition Purchase of one hospital by another
- Provider Consolidation Horizontal Consolidation Hospital to hospital Vertical Consolidation Hospital to physician practice Hospital to long-term care Hospital/physician group to payer
- Reasons for Consolidation Economies of Scale As the size of the organization increases the average cost of producing the good declines Specialization of labor Efficient use of capital Lower input prices for buying in bulk HITECH New forms of financing Accountable Care, Bundled Payment and other forms of capitation Consolidations lead to lower costs, benefit consumers
- Reasons for Consolidation “Hospitals with private rates below 160 percent of Medicare will have difficulty” Journal of Healthcare Management
- Reasons for Consolidation Bargaining power If consolidation helps hospitals by allowing them to negotiate better rates from payers, then this is not good for the consumer. From the hospital’s perspective it doesn’t matter if it is economies of scale or bargaining power, but from society’s perspective it matters
- Coordination vs. Competition Coordination Essential for delivering high quality care Breaking down the silos Competition Essential for innovation and driving higher value There needs to be a balance If coordination leads to integration that can reduce competition Need to watch quality and quantity as well as price
- Hospital Pricing Hospital pricing has received much attention lately Prices that private plans pay are opaque to both consumers and to payers Details of contracts are kept secret Complexity of medical care Employers and employees pay the prices but are not aware of the contract details Silos in health care
- Hospital Pricing
- Hospital Pricing
- Hospital Pricing It is clear that high prices lie at the heart of the health spending problem in the US We don’t fully understand why prices vary across services and across providers. Research from the Center for Studying Health System Change, September 2013 Examined 13 metropolitan areas
- Hospital Pricing High degree of variation in pricing both within and across markets Larger for outpatient than inpatient 5 of the 13 markets are in Michigan which has an unusually concentrated insurance market One insurer has 70% of market share Yet even here there is large variation
- Solutions? Reference Pricing Payer sets a maximum amount for a specific procedure Other “value based” insurance contracts “Nudge” consumer to high value providers Return to selective contracting Regulation All-Payer Model Price Transparency

More Related