Tracheostomy Care for School Nurses
890 likes | 5.04k Views
Tracheostomy Care for School Nurses. Jo Anne Wright, RN, MSN, CNS Pediatric Pulmonary and ENT Trach Nurse Specialist Children’s Hospital/UHHSC. What is a tracheostomy?.

Tracheostomy Care for School Nurses
E N D
Presentation Transcript
Tracheostomy Care for School Nurses Jo Anne Wright, RN, MSN, CNS Pediatric Pulmonary and ENT Trach Nurse Specialist Children’s Hospital/UHHSC
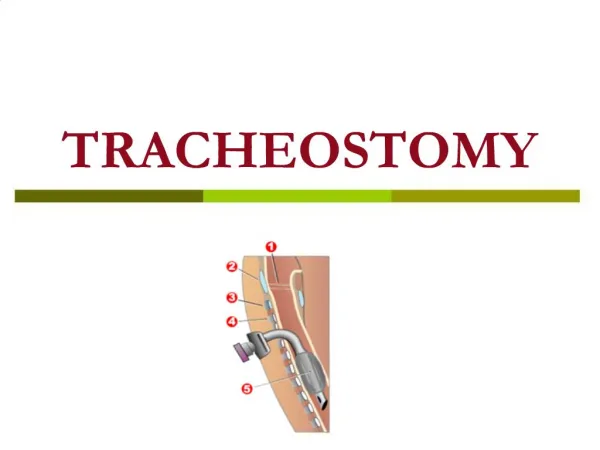
What is a tracheostomy? • Tracheostomy is a surgical procedure that is usually done in the OR under general anesthesia. A tracheostomy is an incision into the trachea that forms a temporary or permanent opening. The terms tracheotomy and tracheostomy are interchangeable. The opening is called a “stoma”.
Indications for a Tracheostomy • Tumor • Stenosis: subglottic, tracheomalacia • Congenital abnormalities of the airway: large tongue or small jaw • Broncho Pulmonary Dysplasia • Chronic pulmonary disease • Chest wall injury • Diaphragm dysfunction
Indications for a Tracheostomy • Neuromuscular diseases, paralysis or weakening chest muscles and diaphragm • Aspiration related to muscle or sensory problems in the throat • Congenital central hypoventilation or central apnea
Types of Tracheostomy Tubes • Single-cannula tubes: used in children, • Double-cannula tubes: inner and outer cannula for older children and teens • Tubes made from plastic or silicone • Cuffed versus uncuffed, aire cuff vs water-filled cuff
Tracheostomy Complications • Mucus plugs are the most common cause of respiratory distress for children with tracheostomies. Symptoms of mucus plug include resistance when trying to suction or bag and/or signs of respiratory distress.
Complications, continued • Bleeding R/T infection, suctioning: too deeply, too aggressively, too much pressure, lack of humidity • Infection R/T pseudomonas, staph, strep, fungus
Symptoms of Respiratory Distress • Cyanosis at the mouth • Struggles at breathing • Clammy skin, • Restlessness • Fingernails cyanotic
Symptoms of Respiratory Distress • Anxiety, frightened look • Retractions • Flared nostrils • Change in pulse or blood pressure
Suctioning a Tracheostomy • The upper airway warms, cleans and moistens the air we breathe. The trach tube bypasses these mechanisms, so that the air via the tube is cooler, dryer and not as clean. In response to these changes, the body produces more mucus. The trach tube is suctioned to remove mucus from the tube and trachea to allow for easier breathing. Generally, the child should be suctioned every 4-6 hrs and as needed.
Suctioning a Tracheostomy • The size of the suction catheter depends on the size of the tracheostomy tube. Size 8 Fr or 10 Fr are typical sizes for pediatric trach tubes. • The catheter should be the largest that fits the trach tube size. • Suction pressure: >1 yr = 100-120 mmHg
More suctioning hints • Shallow suctioning: Suction secretions at the opening of the trach tube that the child has coughed up. • Pre-measured suctioning: Suction the length of the trach tube. Suction depth varies depending on the size of the trach tube. The obturator can be used as a measuring guide.
Deep Suctioning: Insert the catheter until resistance is felt (Deep suctioning is usually not necessary). Be careful to avoid vigorous suctioning, as this may injure the lining of the airway.
Signs that a Child Needs to be Suctioned • Rattling mucus sounds from the trach • Fast breathing • Bubbles of mucus in trach opening • Dry raspy breathing or a whistling noise from trach • Any sign of respiratory distress
More symptoms • Difficulty or refusing to eat • Reduced airflow through the tube • Low O2 saturations
Six Simple Words • WHEN IN DOUBT, CHANGE IT OUT! • WHEN IN DOUBT, CHANGE IT OUT!
Changing the Trach Tube • Insert the new tube in a smooth curving motion directing the tip of the tube toward the back of the neck in a downward and inward arc (like inserting a suction catheter). DO NOT FORCE THE TUBE!!!
Tracheostomy Humidification The nose and mouth provide warmth, filtering and moisture for the air we breathe. A trach tube by-passes these mechanisms. Humidification must be provided to keep secretions thin and to avoid mucus plugs. Children with trachs do best in an environment of 50% humidity or higher. Having humidification is important during sleep. And since we live in the desert, the kids need extra moisture.
Heat Moisture Exchange (HME) or artificial nose • Can be worn 3-4 hrs a day, at least twice a day. • Discard them after use
Tracheostomy Care • Rubbing of the trach tube and secretions can irritate the skin around the stoma. • Trach dressings are used if there is drainage from the trach site or irritation from the tube rubbing on the skin.
Accidental Decannulation • Try to stay calm • Reinsert tube immediately even if conditions are not ideal • There should always be two spare trachs with the child at all times; the child’s size and one size smaller. If the regular size doesn’t fit, then the smaller one will keep the airway patent.
Accidental Decannulation • Opening the airway is always the first priority. If a spare trach tube is not handy, replace the one that came out. You can replace with a clean one later.
Accidental Decannulation • If you can’t reinsert the tube, observe the child to see if he/she can breathe through the stoma itself. This may be possible if the stoma is well healed and fairly large. The child may also be able to breathe through the nose and mouth if there is no severe obstruction above the trach site.
Eating with a Tracheostomy • Having a trach usually will not affect the way a child eats or swallows. Children with isolated airway problems are not likely to have any swallowing problems. • Many kids with trach tubes have GTs, but some take food orally as well.
Speech with a Trach • Normally speech is obtained by a steady stream of air that goes from the lungs and passes by the vocal cords as we exhale. This air is modified by the vocal cords which vibrate as the air passes through to produce sound. Speech production may be affected when a child has a trach because the trach tube re-routes some or all of the exhaled air stream away from the vocal cords.
Natalia uses a Passy Muir speech valve A speech valve is a one-way valve that allows air in, but not out. This forces air around the trach tube, through the vocal cords and out the mouth upon expiration, enabling the child to vocalize.
Ways to Achieve Vocalization with a Trach • Plugging the trach tube by holding a finger or place a cap over the tube for short periods of time. • The child may learn to cover the trach with his/her chin or finger when talking.
How can they talk?With speech Valves Passy-Muir Speech Valves Tracoe Speech Valve
Caps also offer a way to speak Some children have caps over their trach tubes. This causes them to be breathing totally through the nose and mouth. With this in mind, they have vocalization as air passes through the vocal cords as they exhale. DO NOT ALLOW TO SLEEP WITH CAP ON!
After Decannulation • The stoma begins closing as soon as the trach tube is removed. • This may take months to achieve final closure. • Until closed by nature or surgery, need to keep opening covered. • Bandaids work nicely for this; change as needed.
Child may still have mucus coming from the tracheocutaneous fistula. • Must avoid contact with water as this leads directly to the lungs as when the trach tube was in place. • Usually the child will need to have ENT surgery to close the layers if not closed by 1 year.
CPR to a child with a trach tube 1. Suction first. Suction two times. Often this is enough to clear the airway. 2. Call for help and Call 911. 3. No response. Use rescue bag to trach. 4. Get ready to change the tracheostomy tube, if it hasn’t been done yet. 5. No response. Get ready to initiate full CPR with chest compressions after checking for pulse and you find it’s absent.
Emergency Bag of Goodies“Go Bag” Items that should come from home when a child has a trach tube Portable suction Catheters for suctioning trach Catheters or Yankauer tips for oral suctioning Same size trach tube (in box) One size smaller trach tube (in box)
Trach Ties (may be velcro, may be twill tape or metal chain) Water to rinse tubing after suctioning Pre cut 2x2 or 4x4 gauze Extra artificial noses (HME’s) Normal saline bullets (for suctioning)
When the child is discharged from the University Hospital with a trach tube, I generally set up this first bag of goodies. • It’s then up to the parents or caregivers to replace used items.
If these items are not with child, ask parent to send them daily. You need to have equipment available to care for this child. Schools are not responsible for buying this stuff.
If the child is oxygen dependent, should have portable oxygen and a portable pulse oximeter with them. • The oximeter doesn’t need to be a constant monitor unless there are concerns for resp. distress. Periodically, check the O2 sat. It should be >92%.
Ventilatory Dependent Children Two most popular kinds of ventilators used: Pulmonetics LTV 950 Has better ability to offer fine tuning to vent settings
Newport HT 50 Is an older model, less able to fine tune for vent settings.
Important things to know about the vents Generally, the child with severe disabilities and vent dependence is in school for short periods of time. Usually, this child comes with a parent or a home nurse. The school nurse would be extra hands in case of an emergency.
Some children are totally vent dependent and can’t breathe without support. These kids don’t do well “off the vent”. These kids need immediate action. • Some children are able to breathe on their own and use the vent for supplemental support. These kids may be “off the vent” for short periods of time. You have time to figure things out.