Download
1 / 29
290 likes | 558 Views
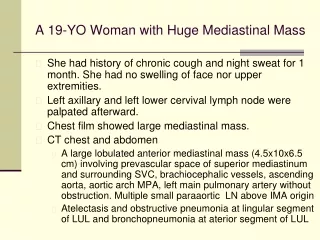
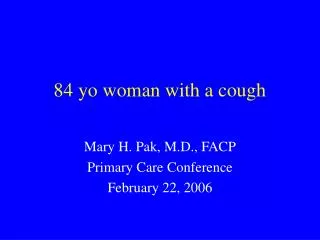
84 yo woman with a cough. Mary H. Pak, M.D., FACP Primary Care Conference February 22, 2006. Disclosure. Received honorarium for being on an advisory panel for Pfizer related to linezolid. Case presentation.

E N D
84 yo woman with a cough Mary H. Pak, M.D., FACP Primary Care Conference February 22, 2006
Disclosure Received honorarium for being on an advisory panel for Pfizer related to linezolid.
Case presentation • EG is an 84 yo woman who presented to the ER with a cough of 1-2 weeks in duration. • She notes some shortness of breath, mostly related to the coughing fits as well as intermittent chest pains. • There is no sputum production. • She has had difficulty sleeping because of the coughing. • She has some nausea related to the cough but no emesis.
Case presentation (con’t) • PMH: Metastatic renal cell CA (treated in eastern Europe, s/p nephrectomy 6 years ago) Hypertension Arthritis Depression
Case presentation (con’t) Medications: captopril 50 mg po b.i.d. Ambien prn Robitussin (OTC) Tylenol prn Allergies: Morphine nausea SH/FH: widowed, lives with daughter in Madison. Denies any tobacco or alcohol use. FH heart disease, no other cancers. No information about her immunization history.
Case presentation (con’t) ROS: No fevers, chills or sore throat No sputum production or hemoptysis No known sick contacts Irritated and itchy eyes occasionally Diffuse arthralgias
Case presentation (con’t) Physical Examination • T 98.9, BP 145/64, pulse 70, resp 16, 95% RA • Lungs were clear to auscultation B/L • Heart was regular in rhythm with no appreciable gallops, murmurs or rubs • Extremities were noted to have trace ankle edema with negative Homan’s sign
Case presentation (con’t) Laboratory data: • WBC 8.1 (normal diff), H/H 11.5/33, plt 285 • Normal electrolytes, creatinine 1.7, BUN 40 • BNP 175 • Troponin 0.1 • D-dimer 0.6
Case presentation (con’t) • Differential diagnosis: • viral URI (including RSV, adenovirus) or URI symptoms related to Influenza type virus • atypical respiratory infections including Mycoplasma pneumoniae, Chlamydia pnueumoniae, Bordetella pertussis, Bordetella parapertussis • Cough secondary to post nasal drip • GERD
Case presentation (con’t) • We sent off a nasopharyngeal swab for Bordetella pertussis DNA PCR and culture • Placed the patient in respiratory droplet isolation • Started azithromycin 500 mg
Objectives • Case presentation • Differential diagnosis of prolonged cough • Discussion regarding epidemiology, diagnosis and treatment of pertussis • Role of adult vaccination
Bordetella pertussis: epidemiology • 25,827 cases reported in the U.S in 2004 • 60% cases in adolescents (11-18) and adults (>20) • Transmitted from person-to-person through aerosolized respiratory droplets from cough or sneeze or direct contact with secretions from infected persons. • Incubation period 5 – 21 d (typical 7 – 10d) • Endemic in U.S., epidemic every 3 - 4 years. Tiwari T, MMWR 2005
Bordetella pertussis: economics • Pertussis in adults has been shown to generate medical and nonmedical costs of $773 per case-patient. • Often leads to 10 days of missed work. Lee GM, Clin Inf Dis 2004
Bordetella pertussis • Uniquely human pathogen • Only disease for which universal childhood vaccination is recommended that has an increasing trend in reported cases in U.S. • In early vaccine years (1920 – 40), average annual rate 150 per 100,000 population • After universal vaccination during 1940’s, declined to 1 case per 100,000. • In 2004, 8.4 cases per 100,000 Robbins JB, Clin Inf Dis 1999 Tiwari T, MMWR 2005
Bordetella pertussis: clinical manifestations • Catarrhal period (1 – 2 weeks) • Coryza, mild fever, non productive cough • Infants can have apnea and respiratory distress • Paroxysmal period (2 – 6 weeks) • Paroxysmal cough, inspiratory “whoop”, posttussive vomiting • Convalescent period (> 2 weeks) Tiwari T, MMWR 2005
Bordetella pertussis: clinical manifestations • Potential complications: • Weight loss (due to coughing) • Sleep disturbance • Effects generated by increased pressure due to severe coughing including pneumothorax, epistaxis, subconjunctival hemorrhage, subdural hematoma, rib fracture, urinary incontinence. • Secondary bacterial pneumonia including aspiration pneumonia related to posttussive vomiting Dworkin MS, Ann Intern Med 2005 Tiwari T, MMWR 2005
Bordetella pertussis: testing • Culture of the nasopharyngeal mucus is the “gold standard” • Prefer aspiration samples via hand-trap • If swabs are to be used, Dacron is recommended since alginate may inhibit PCR-based assays and cotton may be toxic to the bacteria. • Send for B. pertussis PCR and culture. Dworkin MS, Ann Intern Med 2005
Bordetella pertussis: diagnostic barriers • Reluctance to cause patient discomfort • Need for special transport medium (Bordet-Gengou medium) • Tendency for the organism to die before culture confirmation • Low yield of PCR and culture in the setting of partial immunity • Chronicity of cough delays diagnosis to a time when diagnostic yield is poorest. • Lack of reliable serologic markers Dworkin MS, Ann Intern Med 2005
Testing for pertussis is not sufficiently sensitive for treatment decision to be guided by test results alone.
Bordetella pertussis: treatment Tiwari T, MMWR 2005
Bordetella pertussis: vaccination • In May, 2005, Boostrix (GlaxoSmithKline) was licensed for vaccination in persons between the ages of 10 – 18. • In June, 2005, Adacel (Sanofi-Aventis) was licensed for use in person between 11 – 64 years. • Both vaccines are Tdap vaccines which contains tetanus, diphtheria and acellular pertussis. MMWR 2005; 54 (50)
Bordetella pertussis: vaccination • On June 30, 2005, the Advisory Committee on Immunization Practices (ACIP) recommended a single dose of Tdap for all persons aged 11 – 18 years. • In October, 2005, ACIP recommended a single dose of Tdap for adults aged 19 –64. • No adoption into immunization guidelines as yet.
Conclusion • Pertussis is not solely a childhood disease. Pertussis is a “community-acquired disease of all ages” • Reported cases of pertussis has been rising significantly particularly in the adolescents and adults. • Diagnostic testing is not always reliable. Presumptive treatment with a macrolide is recommended. • Additional vaccinations in adulthood might help to decrease the reservoir of pertussis.
References • Dworkin MS. Adults are Whooping, but Are Internists Listening? Ann Intern Med 2005; 142: 832-835. • Tiwari T, Murphy TV, Moran J. Recommended Antimicrobial Agents for the Treatment and Postexposure Prophylaxis of Pertussis: 2005 CDC Guidelines. MMWR 2005; 54 (RR-14): 1- 15. • Pertussis – United States, 2001 – 2003. MMWR 2005; 54 (50): 1283-1286. • Cherry JD. Epidemiological, Clinical and Laboratory Aspects of Pertussis in Adults. Clin Inf Dis 1999; 28 (Suppl 2): S112-S117. • Keitel WA. Cellular and Acellular Pertussis Vaccines in Adults. Clin Inf Dis 1999; 28 (Suppl 2): S118-S123. • Gardner P. Indications for Acellular Pertussis Vaccines in Adults: The Case for Selective Rather than Universal Recommendations. Clin Inf Dis 1999; 28 ( Suppl 2): S131-S135. • Orestein WA. Pertussis in Adults: Epidemiology, Signs, Symptoms and Implications for Vaccination. Clin Inf Dis 1999; 28 (Suppl 2) S147-S150.
References (con’t) 8) Ward JI, et al. Efficacy of an Acellular Pertussis Vaccine among Adolescents and Adults. N Eng J Med 2005; 353: 1555-1563. • Robbins JB. Pertussis in Adults: Introduction. Clin Inf Dis 1999; 28 (Suppl 2): S91-93. • Hewlett EL. A Commentary on the Pathogenesis of Pertussis. Clin Inf Dis 1999; 28 (Suppl 2): S94-S98.