Download
1 / 53
530 likes | 593 Views
Learn about cardiovascular risk factors, atherosclerosis pathology, common diseases, and physiology. Understand venous and arterial supply, atherosclerosis development, MI, PVD, and more.

E N D
CVS Phase 1A The Peer Teaching Society is not liable for false or misleading information…
Aims • Describe the main risk factors in cardiovascular disease • Understand the pathology of atherosclerosis • Understand the main diseases that affect the CVS The Peer Teaching Society is not liable for false or misleading information…
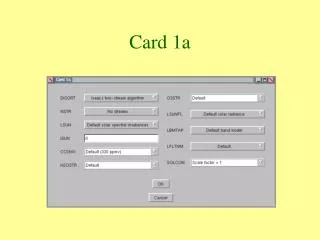
R Common Carotid L Common Carotid Branches of the Aorta L Subclavian R Subclavian Aorta Brachiocephalic DIAPHRAGM Coeliac Inferior Phrenic Splenic L Gastric Hepatic Renal Superior Mesenteric Testicular/Ovarian Inferior Mesenteric Common Iliac The Peer Teaching Society is not liable for false or misleading information…
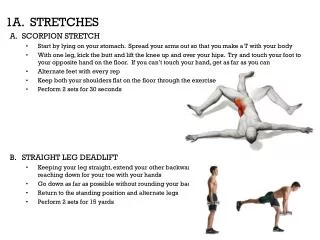
Aorta Arterial Supply of the Lower Limb Common Iliac External Iliac Common Femoral GROIN Deep Femoral Superficial Femoral Popliteal Artery KNEE Peroneal Anterior Tibial Posterior Tibial ANKLE FOOT The Peer Teaching Society is not liable for false or misleading information…
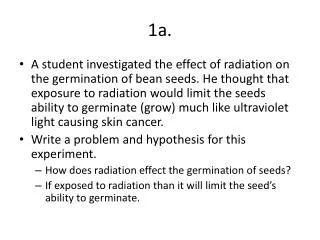
Venous Drainage of the Lower Limb • DEEP vs. SUPERFICIAL VEINS • Blood drains from superficial to deep veins via the perforating veins • Superficial Veins • Great Saphenous – runs up medial side of leg and thigh to join the femoral vein at the saphenous opening • Short Saphenous – drains postero-lateral aspect of the leg and joins the popliteal vein behind the knee The Peer Teaching Society is not liable for false or misleading information…
Physiology BP = CO x PVR • Mean Arterial Pressure (MAP) determines the pressure of blood entering the tissue • Systolic Pressure (SP) = max. arterial pressure occurring just before contraction • Diastolic Pressure (DP) = min. arterial pressure occurring just before ventricular contraction MAP = DP + 1/3(SP-DP) The Peer Teaching Society is not liable for false or misleading information…
Atherosclerosis • Harderning and thickening of arteries which reduces their elastic properties • Involves the formation of an atheroma within the walls of the vessel • Results in a ↓ in the arterial lumen diameter and a ↓ in end-organ perfusion • There is also a predisposition to rupture and thrombus formation The Peer Teaching Society is not liable for false or misleading information…
Atherosclerosis Endothelium damage, LDL moves into intima Fatty STREAK Monocytes migrate into intima and become macrophages, take up LDL and become foam cells. Platelets adhere to endothelial cells, release PDGF, causes smooth muscle migration into intima FIBROLIPID PLAQUES Lesion develops, pressure causes the media to atrophy and the muscle to be replaced by collagen. Fibrous cap of collagen forms. There is ↑ free lipid in the plaque Endothelium become fragile and ulcerates Complicated PLAQUE Further platelet aggregation and thrombus formation The Peer Teaching Society is not liable for false or misleading information…
MI and Angina Underlying pathology and risk factors is the same egatheroslcerosis • Angina: Reduction in blood flow • Can be made better via GTN • Central chest pain and radiation, SOB, variable triggers • Myocardial infarction: Plaque rupture • STEMI/NSTEMI • As above not relived by GTN, may have no precipitations Consequences: Heart failure, infarction, arrthymia’s, depression, decreased ADL’s. The Peer Teaching Society is not liable for false or misleading information…
Peripheral Vascular Disease • = obstruction of large arteries (not within the coronary, aortic arch or brain vasculature) • Main cause is atherosclerosis • Risk Factors • Smoking(!), diabetes, HTN, sedentary lifestyle, ↑cholesterol, obesity • Investigations • Bloods, ABPI, arterial duplex, MR angiography • Management • Conservative measures – lose weight, ↑exercise, anti-hypertensives, statins, STOP SMOKING • Surgery – angioplasty, surgical bypass, amputation The Peer Teaching Society is not liable for false or misleading information…
Intermittent Claudication Cramping pain felt in the calf, thigh or buttock after walking for a fairly fixed distance and relieved by rest = CHRoNIC ISCHAEMIA Ischaemic Rest Pain Burning pain at rest (esp. At night) relieved by hanging legs over the side of the bed + = CRITICAL ISCHAEMIA Ulceration/ Gangrene The Peer Teaching Society is not liable for false or misleading information…1
Venous Thrombosis • Blood clot within veins – generally deep veins of legs (DVT) • Risk factors • Lower limb trauma, surgery or immobilisation in a plaster cast • Bedridden for >3 days or surgery within the last 4 weeks • PMH of DVT/PE • Malignancy • IVDU • Pregnancy • OCP/HRT Vessel Wall VIRCHOW’s TRIAD Blood Constituents Stasis The Peer Teaching Society is not liable for false or misleading information…
Venous Thrombosis • Investigations • D-dimer • Compression USS • Management • Prevention – stop OCP 4 wks pre-op, mobilise pts early, prophylatic anticoagulation • Treatment – Anticoagulation (LMWH then warfarin) • Complications • Pulmonary Embolism - SOB, haemoptysis, pleuritic CP, syncope The Peer Teaching Society is not liable for false or misleading information…
Cardiac physiology Three types of troponin: Troponin C – calcium binds to cause a conformational change in Troponin I. Troponin T – binds to tropomyosin, forming a tropomyosin – troponin complex. Troponin I – binds to actin, to hold the tropomyosin – troponin complexes in place. When calcium binds to troponin C it causes tropomyosin to move out of the way in order to exposure the actin binding sites on the myosin molecules. Therefore enabling the muscle to contract, in the absence of calcium tropomyosin interferes with myosin so the muscle remains relaxed. The Peer Teaching Society is not liable for false or misleading information…
Cardiac physiology VENTRICULAR FILLING (DIASTOLE) • Passive filling of the ventricles – Ventricular volume and pressure increases • AV valves are open • Semi lunar valves are closed ISOVULUMETRIC CONTRACTION (SYSTOLE) • Ventricular pressure> Atrial pressure • Causing the AV valves to close EJECTION (SYSTOLE) • Ventricular pressure> Atrial pressure • Causing the semi lunar valves to open. ISOVOLUMETRIC RELAXATION (DIASTOLE) • Both semi lunar and AV valves are closed • When ventricular pressure < atrial pressure, AV valves open The Peer Teaching Society is not liable for false or misleading information…
Cardiac physiology • Electrical changes in the myocardium • Depolarisation initiated in the SAN which has an inherent rhythm (see later) but also controlled via vagus nerve. It has the fastest rate of discharge in the heart therefore it is the pacemaker, but sometimes other tissue can conduct to the AV node (=ectopics) • Spreads from RA LA causing systole • At AVN the depolarization is delayed by 0.1s so the atria can contract • Conduction continues through bundle of His to its L and R branches • Spreads to purkinje fibres and the rest of the ventricle The Peer Teaching Society is not liable for false or misleading information…
ECG • Detects electrical impulses through the heart • 1 small square = 0.04s • 1 large square = 0.2 s • Use these to work out the heart rate • Check the patient details - is the ECG correctly labelled? • What is the rate? • Is this sinus rhythm? If not, what is going on? • QRS axis • Are the P waves normal (Good places to look are II and V1) • What is the PR interval? • Are the QRS complexes normal? Specifically, are there: • significant Q waves? (seen before R wave- previous MI) • widened QRS complexes? • Are the ST segments normal, depressed or elevated? The Peer Teaching Society is not liable for false or misleading information…
Normal ECG • Regular sinus rhythm 60-100 beats per mintue • P wave (atrial depolarisation) • PR interval 0.12-0.2 s • QRS (ventricular depolarisation) < 0.12s (3 small squares)In general as proceed from V1-6 the R waves get taller and the S waves get smaller • T wave (ventricular repolarisation) The Peer Teaching Society is not liable for false or misleading information…
Normal ECG -90 -30 aVL -150 aVR 0 Lead 1 180 Normal axis LAD RAD 120 Lead 3 90 aVF The Peer Teaching Society is not liable for false or misleading information…
ECG Axis • One quick, non-specific method can be used to determine the QRS axis. When depolaristion moves towards a lead Rwave> S wave i.t QRS is more +ve • If the QRS complex is upright (positive) in both lead I and lead aVF, then the axis is normal • If the QRS is upright in lead I and downward (negative) in lead aVF, then the axis is leftward. • If the QRS is predominately downward in both leads I and aVF, then the axis is rightward. • If the QRS is downward (negative) in lead I and upward (positive) in lead aVF, then the axis is indeterminate. The Peer Teaching Society is not liable for false or misleading information…
Bradycardia’s • Sick sinus syndrome, B-blockers, raised intracranial pressure • AV Block • 1st degree heart block. All atrial pulses reach the ventricle but the conduction is delayed through AV node • ECG: P-R interval > 200ms • 2nd degree heart block. Some atrial pulses reach the ventricaleg not all p waves are followed by a QRS complex • Mobitz type 1: P-R increases over a number of beats followed by an unconducted p wave • Mobitx type 2: P-R interval is constant but QRS complexes are dropped intermittently eg 2:1, 3:1 • 3rd degree heart block. Complete dissociation of p and QRS complexes The Peer Teaching Society is not liable for false or misleading information…
Tachycardia’s • Exercise, fever, anemia, hypovolaemia, emotion, caffiene • Wolf Parkinson white- abnormal conducting pathway between atria and ventricle via an accessory pathway e.g it does not pass through the AV node and so there is no delayed conduction therefore see shortened PR and slurred upstroke in QRS as normal bundle of His pathway catches up • Re-entry tachy • Orthodromic – A.V conduction sets off accessory pathway bypassing AV node- see rapid upstroke and narrow QRS and supressed p wave • Antidromic- Accessory pathway goes back up through AV node. QRS is wide and p wave comes after and is inverted. The Peer Teaching Society is not liable for false or misleading information…
Tachycardia’s • Atrial fibrillation- caused by high firing in the atrium but slower and irregular ventricle response as not all impulses are conducted by the AV node • No p waves • Flutter in V1 • Irregularly irregular rhythm The Peer Teaching Society is not liable for false or misleading information…
Tachycardia’s • Atrial flutter- rapid re-entry of conduction within right atrium. See saw tooth pattern • Ventricular fibrillation The Peer Teaching Society is not liable for false or misleading information…
ST segment elevated (STEMI)/ depressed (ischaemia) The Peer Teaching Society is not liable for false or misleading information…
Bundle Branch Blocks RBBB and LBBB- Delay in conduciton at I.V. Spetum leads to widening of QRS (>120) WiLLiaM (W in V1, M in V6 for LBBB) MaRRow (M in V1, W in V6 for RBBB) The Peer Teaching Society is not liable for false or misleading information…
CVS Reflexes • Aim to maintain mean arterial pressure • Key components: blood vessels, heart and kidney • Pathways controlling MAP • Local eg temperature • Neural control • Vascular reflexes eg stretch leads to contraction • Hormonal factors and local metabolic factors eg angiotensinogen II, NO, K, adenosine CO= HR x SV CO = MAP/TPR The Peer Teaching Society is not liable for false or misleading information…
CVS Reflexes • A volume / arterial BP activation of cardiopulmonary receptors (in atria/ ventricles) / baroreceptors (in aortic arch + carotid sinuses) • Which leads to activation of CNS • Sympathetic tone • Vagal tone • RAS • antiduretic hormone Heart rate + cardiac contractility TPR x CO BP Vasoconstriction Blood volume Na and water excretion, thirst TPR = Total Peripheral Resistance RAS = Renin Angiotensin System Antidiuretic hormone = ADH= Vasopressin The Peer Teaching Society is not liable for false or misleading information…
Shock Inability of CVS to maintain organ perfusion Symptoms: Hypotension, tachcardia, weak pulse, delayed CRP, decreased urine output Signs: Cool skin, low BP, tachyoponea, confusion, thirsty, loss of conciousness • Hypovolaemic: Causes: Trauma, haemorrhage, burns eg rapid fluid loss causing mechanisms to be activated (see above) • Septic: Infection results in release of toxins causing increased permeability • Fever, chills, sweating • Anaphylatic- Severe allergic reaction • angiodema and narrowing of airways • Cardiogenic: Damage to myocytes causing ineffective pumping eg MI The Peer Teaching Society is not liable for false or misleading information…
Cardiac output and Starling’s law • CO = Stroke volume x heart rate • SV is influenced by the filling pressure (preload), the force of the cardiac muscle and the pressure against which the heart has to pump (afterload). • The volume of blood in the ventricle before systole (contraction) is the end diastolic volume. This is dependant on the end-diastolic pressure and the compliance of the ventricle i.e. how easy it relaxes. • If EDP and therefore EDV rises then the force of the next contraction and the stroke volume will increase • = FRANK-STARLING RELATIONSHIP Sympathetic tone contractility normal SV Failure (decreased contractility) The Peer Teaching Society is not liable for false or misleading information… EDP
Cardiac output and Starling’s law • Starlings Law = The energy released during contraction depends on the initial fiber length • The consequence of this is to match left and right ventricular output otherwise if RV>LV it would lead to an increase in pulmonary blood pressure and may result in pulmonary oedema. • Due to starlings law any increase in blood flow would increase the filling pressure and hence EDV within the LV . This would result in an increase in LV output and would prevent any rise in pulmonary pressure. • Therefore an increase in central venous pressure e.g. in exercise will also result in an increased cardiac output, conversely a decrease in central venous pressure eg sitting to standing will lead to a fall in CO The Peer Teaching Society is not liable for false or misleading information…
Heart Failure • Occurs when the heart is no longer able to maintain sufficient tissue perfusion for normal cellular metabolism. Due to, • Damaged cardiac muscle eg IHD • HBP (increased afterload means the heart has to work harder) • valular heart disease (increase afterload and so increase the work of the heart) The Peer Teaching Society is not liable for false or misleading information…
Heart Failure Pathogensis A decrease in LV systolic dysfuction results in a decrease in contractility and shifts the starling curve to the right. This results in a decreased force of contraction. The body then tries to compensate by increasing the filling pressure (EDP). Its does this by • Increased sympathetic activity HR and force • Peripheral vasconstriction EDP (but also afterload!!) • RAS activation Retention of Na and water However these responses eventually overwhelm the heart and prolonged excessive filling leads to dilatation which leads to ineffectual contraction and possible valvular incompetence. Dilation also increase the work of the myocytes (Laplace’s law) thus predisposing the myocardium to ischeamia and damage. This leads to further cardiac remodelling, which leads to a further reduction in CO. The Peer Teaching Society is not liable for false or misleading information…
Heart Failure- Clinically Can get both = Congestive cardiac failure Cor pulmonale = RHF due to chronic pulmonary disease The Peer Teaching Society is not liable for false or misleading information…
Heart sounds The Peer Teaching Society is not liable for false or misleading information…
JVP • Manonmeter of right atrial pressure. Observed with the patient at 45o • Distinguish from carotid artery as it • Multiphasic • Non- palpable • Occludable • Varies with head tilit • Varies with respiration • Elevated due to • Fluid overload • SVC obstruction • RVF • Constrictive pericarditis • Tricuspid stenosis/ regurg a wave represents atrial systole c wave represents closure of the tricuspid valve x descent represens the fall in atrial pressure during ventricular contraction. v wave represents the atrial filling against the closed tricuspid. y descent represents opening of the tricuspid valve. The Peer Teaching Society is not liable for false or misleading information…
Embryology Development of primitive heart • Sinus venosus: Left horncoronary sinus Right horn wall of right atrium • Primitive atrium: Right half right auricle of right atrium Left halfleft auricle of left atrium • Bulbous courdis: Right ventricle/ Outflow of right and left ventricle The Peer Teaching Society is not liable for false or misleading information…
Embryology • Origins of chambers of the heart • Left atrium: is formed from 4 primitive pulmonary veins • Right atrium: primitive atrium and sinus venosus (right horn) • Ventricles: (L)- primitive ventricle, (R)- Bulbous cordis • Pulmonary trunk/ aorta: bulbous courdis/ Truncus ateriosus • SA Node/ AV Node and bundle- sinus venosus/ AV canal • Pericardium- Septum transversum The Peer Teaching Society is not liable for false or misleading information…
Embryology http://www.indiana.edu/~anat550/cvanim/aarch/aarch.html The Peer Teaching Society is not liable for false or misleading information…
Questions • This is the normal duration/range of the QRS complex in msec • This is the normal duration/range of the PR interval in msec • This is the angle/range assessed by limb lead II in degrees • This is the angle/range assessed by limb lead I in degrees • This is the duration/range in msec represented by one small square on a standard ECG recording • This is the duration/range of the QRS complex in msec in lead V6 in an ECG showing complete left bundle branch block • 120 to 200 • Less than or equal to 120 • -30 to 90 • 40 • Greater than 100 • 60 • 0 • 60 to 100 • Greater than 120 • Less than 60 The Peer Teaching Society is not liable for false or misleading information…
Questions • This is the normal duration/range of the QRS complex in msec • This is the normal duration/range of the PR interval in msec • This is the angle/range assessed by limb lead II in degrees • This is the angle/range assessed by limb lead I in degrees • This is the duration/range in msec represented by one small square on a standard ECG recording • This is the duration/range of the QRS complex in msec in lead V6 in an ECG showing complete left bundle branch block • 120 to 200 (2) • Less than or equal to 120 (1) • -30 to 90 • 40 (5) • Greater than 100 • 60 (3) • 0 (4) • 60 to 100 • Greater than 120 (6) • Less than 60 The Peer Teaching Society is not liable for false or misleading information…
Questions Aortic Arch Embryology .For each of the following post-natal structures, indicate their embryological origin. • Ductus Arteriosus. • Aortic Arch. • Left Common Carotid Artery. Left 1st arch Right 2nd arch Left 3rd arch Right 3rd arch Left 4th arch Right 4th arch Left 5th arch Right 5th arch Left 6th arch Right dorsal aorta The Peer Teaching Society is not liable for false or misleading information…
Questions Aortic Arch Embryology .For each of the following post-natal structures, indicate their embryological origin. • Ductus Arteriosus. • Aortic Arch. • Left Common Carotid Artery. Left 1st arch Right 2nd arch Left 3rd arch (3) Right 3rd arch Left 4th arch (2) Right 4th arch Left 5th arch Right 5th arch Left 6th arch (1) Right dorsal aorta The Peer Teaching Society is not liable for false or misleading information…
Questions • A circulating count of less than 80 x 109/L of this blood constituent is associated with increased risk of bleeding whilst an excess is associated with increased risk of thrombosis. • This blood constituent plays the major role in maintaining oncotic pressure and retaining fluid in the intravascular space. • These differentiated B lymphocytes produce antibodies in response to non-self protein antigens. • The number of these in the blood is regulated by erythropoietin • Platelets • Eosinophils • Plasma cells • Monocytes • Erythrocytes • Leukocytes • Albumin • Immunoglobulins • Haemoglobin • Coagulation factors The Peer Teaching Society is not liable for false or misleading information…
Questions • A circulating count of less than 80 x 109/L of this blood constituent is associated with increased risk of bleeding whilst an excess is associated with increased risk of thrombosis. • This blood constituent plays the major role in maintaining oncotic pressure and retaining fluid in the intravascular space. • These differentiated B lymphocytes produce antibodies in response to non-self protein antigens. • The number of these in the blood is regulated by erythropoietin • Platelets (1) • Eosinophils • Plasma cells (3) • Monocytes • Erythrocytes (4) • Leukocytes • Albumin (2) • Immunoglobulins • Haemoglobin • Coagulation factors The Peer Teaching Society is not liable for false or misleading information…
Questions Atherosclerosis. • These cells enter the artery wall in response to chemokines and facilitated by adhesion molecules such as VCAM-1 where they may interact with antigens such as oxidised LDL. • This is the first lesion in the progression from normal vessel wall to obstructive or ulcerating atheroma. • This event underlies the majority of myocardial infarctions and strokes. • This can be quantified in coronary arteries using modern CT scanning methods Platelet aggregation Eosinophils T Lymphocytes Fatty streak Aneurysm formation Plaque rupture Mast cells Macrophages Lipid pool Calcification The Peer Teaching Society is not liable for false or misleading information…
Questions Atherosclerosis. • These cells enter the artery wall in response to chemokines and facilitated by adhesion molecules such as VCAM-1 where they may interact with antigens such as oxidised LDL. • This is the first lesion in the progression from normal vessel wall to obstructive or ulcerating atheroma. • This event underlies the majority of myocardial infarctions and strokes. • This can be quantified in coronary arteries using modern CT scanning methods Platelet aggregation Eosinophils T Lymphocytes (1) Fatty streak (2) Aneurysm formation Plaque rupture (3) Mast cells Macrophages Lipid pool Calcification (4) The Peer Teaching Society is not liable for false or misleading information…
Questions • The SAN is supplied by the RCA in what percentage of people? • The AVN is supplied by the RCA in what percentage of people? • Left dominance of the coronary arteries occurs in what percentage of the population? 10% 20% 40% 60% 70% The Peer Teaching Society is not liable for false or misleading information…
Questions • The SAN is supplied by the RCA in what percentage of people? • The AVN is supplied by the RCA in what percentage of people? • Left dominance of the coronary arteries occurs in what percentage of the population? 10% (3) 20% 30% 60% (1) 90% (2) The Peer Teaching Society is not liable for false or misleading information…
Questions • What is Starling’s law? • A 68 year old presents to his GP with HBP. He is given some medication. Later he goes home but presents to A+E complaining of muscle weakness and aches, muscle cramps and palpitations, he then collapses. • Normal BP range and if diabetic? • Risk factors for high blood pressure? • What class of medication was given? • Where does this act? • How does this account for the gentlemens symptoms? The Peer Teaching Society is not liable for false or misleading information…