Download
1 / 15
150 likes | 264 Views
ACCESS TO AND USE OF FAMILY PLANNING BY WOMEN WITH HIV. IAS, Cape Town Revisiting Contraception and HIV Bridging Session 22 nd July 2009 J Smit, H Rees, M Beksinska Reproductive Health and HIV Research Unit. CONTRACEPTIVE USE PATTERNS.

E N D
ACCESS TO AND USE OF FAMILY PLANNING BY WOMEN WITH HIV IAS, Cape Town Revisiting Contraception and HIV Bridging Session 22nd July 2009 J Smit, H Rees, M Beksinska Reproductive Health and HIV Research Unit
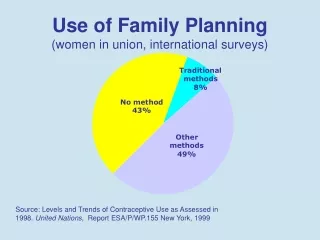
CONTRACEPTIVE USE PATTERNS In sub-Saharan Africa: 14% women (married/in union) use a modern, reversible, highly effective method: OC 4%; IC/implant 6%; IUD 0.5%; Condom 2%; TL 2% World Contraceptive Use 2007. Overall rates and country rates. http://www.un.org/esa/population/publications/contraceptive2007/contraceptive_2007_table.pdf. WHO Reproductive Choices & Family Planning for People Living with HIV: Counselling Tool
CONTRACEPTIVE METHOD MIX *United Nations, World Contraceptive Use 2007
CONTRACEPTIVE USE AMONG WOMEN (15-24yrs), KNOWN HIV STATUS, IN 4 AFRICAN COUNTRIES Leclerc et al, 2008, Hormonal Contraception and HIV in four African countries. Contraception
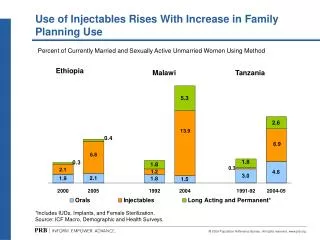
ISSUES FOR HIV INFECTED WOMEN • High unmet need for FP (United Nations, World Contraceptive Use 2007) • Method skew in many Sub-Saharan countries (IC: Malawi, OC: Zim) (Sullivan et al. 2006. Skewed contraceptive method mix: Why it happens, why it matters. J.Biosoc.Sci,) • High IC use in countries with high HIV prevalence (United Nations, World Contraceptive Use 2007) • High IC use amongst young women (Leclerc et al, 2008, Hormonal Contraception and HIV in four African countries. Contraception; 2003SADHS) • Condom use low within marriage/stable relationships (Morrison et al, 2009. Highly effective contraception and acquisition of HIV and other sexually transmitted infections. Best Practice & Research Clinical Obstetrics and Gynaecology.)
WHAT IS AVAILABLE FOR HIV INFECTED WOMEN Fourteen million women with limited options: HIV/AIDS and highly effective reversible contraception in sub-Saharan Africa Stuart G. 2009. Contraception Similar to method mix for all women; often skewed Focus on dual protection Need for highly effective methods • HCs: OCs, ICs, Implants, EC • Cu-IUDs • LNG-IUS • Barrier methods (MC,FC) WHO Reproductive Choices & Family Planning for People Living with HIV: Counselling Tool
WHAT METHODS DO HIV INFECTED WOMEN USE? (%) LITTLE PUBLISHED ON METHODS USED BY HIV INFECTED WOMEN IN AFRICA. THE FOCUS IN THE LITERATURE IS ON FERTILITY INTENTIONS
FACTORS AFFECTING UPTAKE AMONG HIV-INFECTED WOMEN Uptake and continuation issues similar to those for all women • HIV infected women’s desire for children varies • Many women don’t know they are HIV infected • Choosing condoms for contraception allows avoidance of status disclosure; easier to negotiate condoms for FP than disease • Female controlled methods desired – partner more likely to use condoms • Protection against STIs • Whether on ARVs -- DIs • Side effects (e.g. amenorrhoea)
WHAT GUIDANCE DO PROVIDERS GIVE WOMEN WITH HIV? Providers’ preferences can influence contraceptive method mix • Little documented, again focus is on reproductive rights • Attitudes to HIV & fertility influenced negatively by bio-medical concerns • Switch from OC to IC (DI) • Concerns about IC use with ARVs (DI) • Concerns about IUD use in HIV+ women
CONSIDERATIONS FOR METHOD MIX FOR HIV INFECTED WOMEN • Efficacy (DI?) • Side effects • Safety: HIV progression; CI • Acceptability, convenience, discontinuation • potential for inconsistent use • dual protection properties • partner sero-status • female initiated -- need for secrecy/partner approval • Cost A range of methods is needed
Ramkissoon, Smit et al, SA Health Review 2006. Options for HIV Positive Women
GUIDELINES: CONTRACEPTION FOR HIV INFECTED WOMEN • Continue to use hormonal contraceptives in HIV infected women • Generally use hormonal contraceptives with ARVs • Consider drug interactions, especially with rifampicin • Continue to use IUDs in HIV infected women but not for women at individual high risk for STIs • Promote dual method use/ dual protection/ EC • Consider female and male sterilisation, • Consider progestin implants which have better contraceptive SE profile and are long acting WHO MEC, 2004. http://www.who.int/reproductive-health/publications/mec/mec.pdf
WHAT IF HCs WERE FOUND TO INCREASE HIV PROGRESSION? Changes in method provision guidance -- what methods would be appropriate? Changes in contraceptive counseling Messages about increased risk What’s the trade off between offering effective contraception versus avoiding possible increased risk of acquisition or disease progression among HIV infected women, and what’s the best method for HIV infected women?
ARE NEW METHODS NEEDED ? Little attention paid to new methods Highly effective reversible methods were not developed in the context of HIV—OCS, ICs, IUDS developed > 40 yrs ago • New designs of FCs • Microbicides with contraceptive properties • Methods which offer dual protection, are female controlled • Increase awareness/access to EC
CONCLUSIONS Adequate provision of condoms + comprehensive selection of highly effective contraceptive methods is a public health priority Contraceptive guidelines needed for HIV infected people Integrate family planning in HIV services (PMTCT, ARV) “provider initiated family planning” Create appropriate messaging, dispel myths More research: - patterns of use - role of providers in counseling about options - among young women (<25) using HCs Consider reproductive health rights