Download
1 / 1
20 likes | 117 Views
Consider ACE-I/ ARB and Thiazide interventions 48 - 72 hours Post Stroke (sooner with TIAs). 1. History of Orthostasis 2. Current Symptoms 3. Possible Med Interactions 4. Med Contraindications 5. BP measurements 6. Worsening of stroke symptoms in the last 48 hours.

E N D
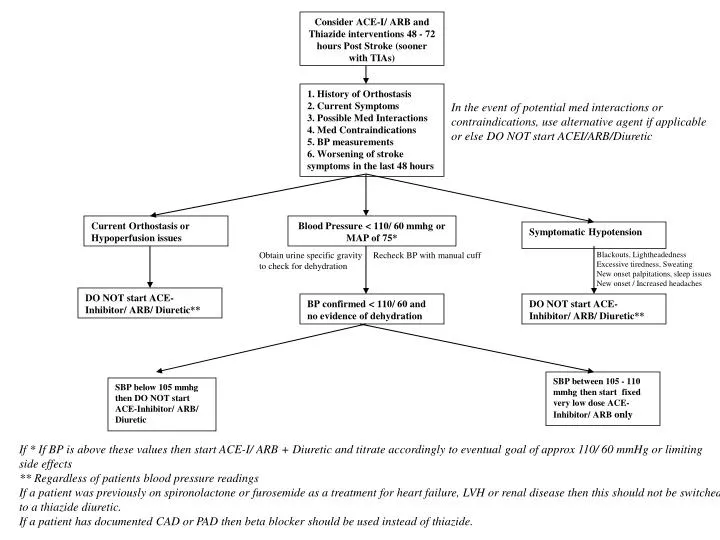
Consider ACE-I/ ARB and Thiazide interventions 48 - 72 hours Post Stroke (sooner with TIAs) 1. History of Orthostasis 2. Current Symptoms 3. Possible Med Interactions 4. Med Contraindications 5. BP measurements 6. Worsening of stroke symptoms in the last 48 hours In the event of potential med interactions or contraindications, use alternative agent if applicable or else DO NOT start ACEI/ARB/Diuretic Current Orthostasis or Hypoperfusion issues Blood Pressure < 110/ 60 mmhg or MAP of 75* Symptomatic Hypotension Obtain urine specific gravity to check for dehydration Recheck BP with manual cuff Blackouts, Lightheadedness Excessive tiredness, Sweating New onset palpitations, sleep issues New onset / Increased headaches DO NOT start ACE-Inhibitor/ ARB/ Diuretic** BP confirmed < 110/ 60 and no evidence of dehydration DO NOT start ACE-Inhibitor/ ARB/ Diuretic** SBP between 105 - 110 mmhg then start fixed very low dose ACE-Inhibitor/ ARB only SBP below 105 mmhg then DO NOT start ACE-Inhibitor/ ARB/ Diuretic If * If BP is above these values then start ACE-I/ ARB + Diuretic and titrate accordingly to eventual goal of approx 110/ 60 mmHg or limiting side effects ** Regardless of patients blood pressure readings If a patient was previously on spironolactone or furosemide as a treatment for heart failure, LVH or renal disease then this should not be switched to a thiazide diuretic. If a patient has documented CAD or PAD then beta blocker should be used instead of thiazide.