Management Guidelines for Chronic Rhinosinusitis with and without Nasal Polyps
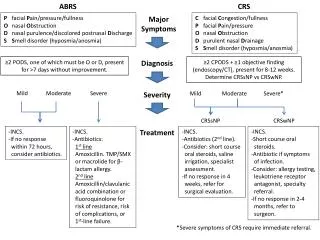
This document provides comprehensive guidelines for the diagnosis and management of chronic rhinosinusitis (CRS) with (CRSsNP) and without nasal polyps (CRSwNP). It delineates diagnostic criteria, including symptom duration and objective findings such as endoscopy or CT scans. Treatment recommendations include the use of intranasal corticosteroids (INCS) and antibiotics based on severity, with instructions for escalation if there is no improvement. Referrals for surgical evaluation or specialty assessment are advised when symptoms persist despite treatment.

Management Guidelines for Chronic Rhinosinusitis with and without Nasal Polyps
E N D
Presentation Transcript
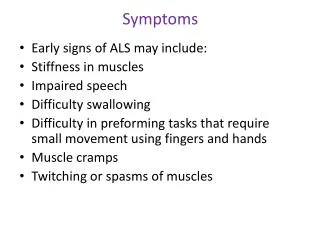
ABRS CRS P facial Pain/pressure/fullness O nasal Obstruction D nasal purulence/discolored postnasal Discharge SSmell disorder (hyposmia/anosmia) Major Symptoms C facial Congestion/fullness P facial Pain/pressure O nasal Obstruction D purulent nasal Drainage SSmell disorder (hyposmia/anosmia) ≥2 PODS, one of which must be O or D, present for >7 days without improvement. Diagnosis ≥2 CPODS + ≥1 objective finding (endoscopy/CT), present for 8-12 weeks. Determine CRSsNP vs CRSwNP. Mild Moderate Severe Mild Moderate Severe* Severity CRSsNP CRSwNP -INCS. -If no response within 72 hours, consider antibiotics. -INCS. -Antibiotics: 1st line Amoxicillin. TMP/SMX or macrolide for β- lactam allergy. 2nd line Amoxicillin/clavulanic acid combination or fluoroquinolone for risk of resistance, risk of complications, or 1st-line failure. Treatment -INCS. -Antibiotics (2nd line). -Consider: short course oral steroids, saline irrigation, specialist assessment. -If no response in 4 weeks, refer for surgical evaluation. -INCS. -Short course oral steroids. -Antibiotic if symptoms of infection. -Consider: allergy testing, leukotriene receptor antagonist, specialty referral. -If no response in 2-4 months, refer to surgeon. *Severe symptoms of CRS require immediate referral.