Download
1 / 42
430 likes | 613 Views
Nur Rasyid Department of Urology Faculty of Medicine University of Indonesia. Role of Urology in Treatment of Male Infertility. Introduction. US & Europe : 20% are unable to conceive 50% : male factor Urologist : first specialist visit for man factor. Aetiology. EAU Guidelines 2005.

E N D
Nur Rasyid Department of Urology Faculty of Medicine University of Indonesia Role of Urology in Treatment of Male Infertility
Introduction • US & Europe : 20% are unable to conceive • 50% : male factor • Urologist : first specialist visit for man factor
Aetiology EAU Guidelines 2005
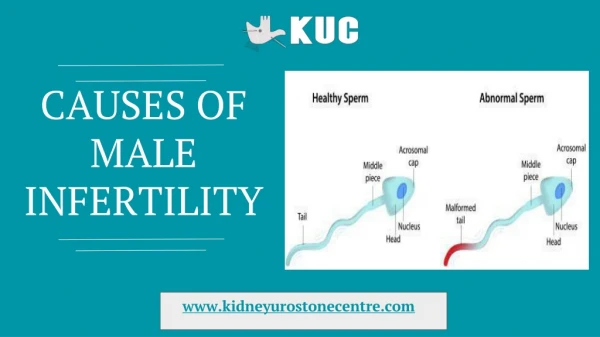
Causes of male infertility in RSCM Taher A. Unpublished data
Aetiology • Pretesticular • Testicular • Post Testicular
Pre Testicular • Hypothalamic disease • Gonadotropin deficiency (Kallmann syndrome) • Isolated LH deficiency (“fertile eunuch”) • Isolated FSH deficiency • Congenital hypogonadotropic syndromes • Pituitary disease • Pituitary insufficiency (tumors, infiltrative processes, operation, radiation, deposits) • Hyperprolactinemia • Exogenous hormones (estrogen-androgen excess,glucocorticoid excess, hyper- and hypothyroidism) • Growth hormone deficiency
Testicular • Chromosomal (Klinefelter syndrome [XXY], XX sex reversal, XYY syndrome) • Noonan syndrome (male Turner syndrome) • Myotonic dystrophy • Vanishing testis syndrome (bilateral anorchia) • Sertoli-cell-only syndrome (germ cell aplasia) • Y chromosome microdeletions (DAZ) • Gonadotoxins (radiation, drugs) • Systemic disease (renal failure, liver failure, sickle cell anemia) • Defective androgen activity • Testis injury (orchitis, torsion, trauma) • Cryptorchidism • Varicocele • Idiopathic
Post Testicular • Reproductive tract obstruction • Congenital blockages • Congenital absence of the vas deferens (CAVD) • Young syndrome • Idiopathic epididymal obstruction • Polycystic kidney disease • Ejaculatory duct obstruction • Acquired blockages • Vasectomy • Groin surgery • Infection • Functional blockages • Sympathetic nerve injury • Pharmacologic • Disorders of sperm function or motility • Immotile cilia syndromes • Maturation defects • Immunologic infertility • Infection • Disorders of coitus • Impotence • Hypospadias • Timing and frequency
Varicocele • Most common correctable cause • Occur 15 % of the general population • Up 35 % of men being evaluated for primary infertility • Up to 80 % of men with secondary infertility • Incompetent venous valve • Associated a progressive and time-dependent deterioration in testicular function
Varicocele Repair • Retroperitoneal • Open (Palomo procedure) • Laparoscopic • Inguinal (Ivanisevich procedure) • Using Lense Loupe or Microscope • Subinguinal
Improvement • Semen quality improvement : 60 – 80 % • Pregnancy rate : 20 – 60 %
Endocrinopathies Only EAU Guidelines 2005
Endocrinopathies • Disorder of production or secretion of GnRH • Disorders of pituitary function • Disorders of testosterone synthesis and function
Disorder of production or secretion of GnRH Disorders of pituitary function Disorders of testosterone synthesis and function
Disorder of production or secretion of GnRH • Low levels of FSH and LH • Kallmann’s syndrome • Hormonal replacement with hCG
Disorders of pituitary function • Pituitary mass • Direct compression of the portal system • Decrease FSH/LH secretion hypogonadotropic hypogonadism • Must performed imaging to find pituitary adenoma • Sugical, radiation and medical (cabergoline, bromocriptin) treatment
Disorders of testosterone synthesis and function • Defect enzym for systhesis testosterone • Defect Androgen receptor • Exogenous androgen reversible in 6 month to 1 year • Treatment • Testosterone supplement • Aromatase inhibitor • Antiestrogens
Cryptorchidism & Orchiopexy • Histopathologic hallmarks • Decreased numbers of Leydig cells, • Degeneration of Sertoli cells • Delayed disappearance of gonocytes, • Delayed appearance of adult dark (Ad) spermatogonia • Failure of primary spermatocytes to develop • Reduced total germ cell counts
Cryptorchidism & Orchiopexy • Also increase malignancy risk • Treatment : • Orchiopexy in 1 year of age
Disorders of ejaculation • Failure of emission or ejaculation • Symphatic nerves injury • Retrograde ejaculation • Medication, prior surgery to bladder neck
Disorders of ejaculation • Treatment • Neurogenic problem : simpathomimetic agents enhance emission and close bladder neck (successful in 50 % cases) • Post ejaculate-urine specimen • Vibratory stimulation under anaesthesia • If all above fail IVF / ICSI
Obstruktif Azoospermia • Tidak adanya spermatozoa dan sel spermatogenesis pada semen dan urine pasca ejakulasi yang disebabkan oleh sumbatan bilateral pada duktus seminalis
Obstruction Depend level of obstruction • Complete ejaculatory duct obstruction • Low Volume, acidic, fructose negative ejaculate • Vasa or epididimis obstruction • Normal volume, basic, fructosa positive ejaculate
Vasal obstruction • Most common etiology : post vasectomy • Treatment • Modified single layer vasovasostomy • Two layer vasovasostomy • Vasoepidimostomy
Congenital bilateral absence of the vas deferens • Sperm harvested from • Epididymis (MESA) • Testis (TESE) • ICSI
Conclusion • Each infertility case must be examine carefully to select spesific treatment • Urologist has a pivotal role in surgery treatment for infertility cases