Download
1 / 85
900 likes | 1.67k Views
Faculty of Pharmacy , Lille II Friday 12th, February 2010. Therapeutic Approaches to Skin Pigmentation Disorders. Pauline Fontaine Clotilde Bourdon Antoine Henninot. 5 main functions:

E N D
Faculty of Pharmacy, Lille II Friday 12th, February 2010 Therapeutic Approaches to Skin Pigmentation Disorders Pauline Fontaine Clotilde Bourdon Antoine Henninot
5 main functions: • Barrier : Langerhans cells + Sebaceous glands + Melanocytes+ Hair follicles • Sens of touch, sensation : Nerve endings Merkel cells • Regulates body temperature • Excretes waste product and excess salt • Syntheses vit D • Skin appendages: hair, nails, sweat glands, sebaceous glands • CAUTION WITH THE TARGETS • TOUGH TO PENETRATE The skin: an heterogeneous system
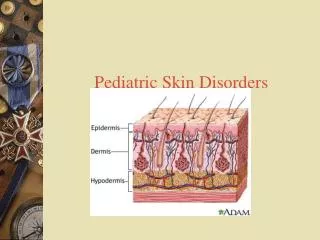
Epidermis • Skin's outer structure • Stratified • Stratum corneum= outermost layer, dead cells: not permeable • Keratinocytes (++), melanocytes, Langerhans cells, Merkel cells • Melanocytes(5% of the cells) • Avascular
Dermis • Melanocytesunderneath the basal layer i.e. within the dermis • Contains: - blood vessels - lymph vessels - hair follicles - glands (produce sweat and sebum) => Rich capillary bed for systemic drug absorption
3 major routes to entry into the skin • Sebum and surface material (1) • Skin appendages (3) • Epidermal route (2) -> Inter- or trans-cellular route Hydrophilic + Lipophilic substances Lipophilic substances
Figure 1. Simplified representation of skin showing routes of penetration: (1) through the sweat ducts; (2) directly across the stratum corneum; (3) via the hair follicles.Reproduced with permission from Ref 10.
Origin of cutaneous pigmentation • Skin color determined by its content in pigments • Melanins +++++, • Oxygenated and reduced hemoglobin • and Carotene • Other factors • epidermal thickness • vascular supply
Synthesis of Melanins • In the melanocytes, within melanosomes • Through fixation of α-MSH on MC1R • with UVB rays • Melanins absorb UV rays => protection
α-Melanocyte-Stimulating Hormone Hypophysis • Peptide • endogenous agonist for all Melanocortin Receptors • regulator of skin and hair pigmentation • Short t1/2 in circulation Synthesis/Secretion Hydrolysis
POMC ACTH Melanocyte ↗AMPc Eumelanin + α-MSH + - - ↘AMPc Phemelanin MC1R ASIP
Tyrosinase Glutathion ou Cystein TRP1 TRP2 Eumelanin Phaeomelanin
Melanosome migration withinmelanocytes => Maturation (polymerisation)
Melanocytes Black skin White skin Similar number of melanocytes BUT melanin synthesis and melanocytes’ migration to the keratinocytesmore significant for black skin
Faculty of Pharmacy, Lille II Friday 12th, February 2010 DERMATOLOGICDISORDERS Pauline Fontaine Clotilde Bourdon Antoine Henninot
Overview of the diseases Pregnancy mask • Vitiligo
Hyperpigmentation disorders • Unknownetiologicorigin • High prevalence • Lentigo: 90% of the population over 70 • Melasma (chloasma): 8.8% of the latino americanwomen • Alter people’squality of life • Melasma: reemergence of the lesions as soon as the first exposition to the sunlight
Melasma Lentigo
Currenttreatments • Oldbleaching agents • Hydroquinone (tyrosinase inhibitor) • Azelaicacid • Corticoïd • Associatedwith« peeling » / dermabrasionproducts • Vitamin A • Glycolicacid • Best treatment: Kligman trio • Corticoïd (dexamethasone) • Hydroquinone • Retinoicacid
Currenttreatments (continued) • SatisfyingBUT: - unconstanttreatment - local treatmentvery long - numerousAdverse Events : irritation (hydroquinone (5%), retinoicacid) • Depigmenting duo: hydroquinone corticoid (hydrocortisone) less irritant BUT less effective • => B/R ratio NOT acceptable for skin disorders • 1st TREATMENT= SOLAR PROTECTION!!!
Meeting withDr.Riboulet, Dermatologist Main ideas: • Keratolytic peeling : caution with the concentration, otherwise -> inflammation, post –inflammatory hyperpigmentation • Total depigmentation with MBEH (Mono Benzyl Ether Hydroquinone) prohibited in France to treat Melasma -> too hazardous • Whitening agent : undesired hypopigmentation risk
Hypopigmentationdisorders • Vitiligo • High prevalence: 0.5 - 2% of the population • Unknownetiology • 3 major hypotheses, not exclusive of each other: • immunologicfactors • oxidative stress • sympathetic neurogenic disturbance
Currenttreatments • Puvatherapy (psoralen + UVA) no longer used (knowncarcinogenicrisk) • UVB narrow band • For 10 years: unknownrisk cancer • Topicaltreatments • Tacrolimus (off label) • Corticoïd • Surgery: too invasive technique • If spot entirelyhealed, no relapsing
Meeting withDr.Riboulet, Dermatologist • « patients with vitiligo have a bad observance withtheirtreatmentsbecausethey are restrictive and difficult. There isthendefinitely a market for new efficacioustreatments » • « So oldtreatments! » • « Camouflage »
Meeting withDr.Riboulet, Dermatologist Conclusion : • patients disappointed with their treatments • the market exists, patients are waiting for efficacious treatments => new potential targets exploration
Real diseases or just quality of life? • Skin =body's envelope, reactions and emotions expressed via the skin • Means of exercising power over others, captivating, influencing impressions and judgement, conquering • Significantpsychological impact • Dermatology Life Quality Index (DLQI)
Reasoning • list of potentialtargets for each indication (hypo- + hyper- pigmentation) • For eachtarget • Location • Advantages / Inconvenients • Drugs on the market • Target’smechanism of action • Is the targetinteresting??? • If YES => development
Hypopigmentation α-MSH Synthesis • POMC • Central action • Involvedtooearly in the α-MSH pathway and involved in toomanysignallingpathways • ACTH • Central + Peripheral actions • Involved in toomanysignallingpathways • Production of mineralocorticoids, glucocorticoids, androgens by the surrenal glands schema 1.pdf
Hypopigmentation Action on MC1R • α-MSH • Action on the differentMCRs (MC1R) • Activation of melanogenesis • Anti inflammatoryeffect • MC1R • Present on inflammatorycells and melanocytes • Rolewithinmelanocytes: melanogenesisalone
POMC ACTH Melanocyte ↗AMPc Eumelanin + α-MSH + - - ↘AMPc Phemelanin MC1R ASIP
MC1R belongs to the MCRsfamily • 5 G-protein-coupled transmembranereceptors (MC1R-5R), • Positively coupled to adenylylcyclase
Ideas to develop for Vitiligo • MC1R : preferentialtarget Type b receptorsverydifficult to screen EXCEPT for MC1bR!!! MC1R: Peptide Rcwith an externalloop (≠ OpiateRcs)
Action on MC1R • Agonist MC1R discovered by BMS • Peptidicagonist: Melanotan I Ac-Ser-Tyr-Ser-NorLeu-Glu-His-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH2
Someotherpeptidicagonists • 1) Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Ava-Lys-Pro-Val-NH2 Ava9-10-NDP-αMSH • 2 ) Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg–Gly-Lys-Pro-Val-NH2 desTrp9-NDP- α MSH
Clinical trials of Melanotan I • Subcutaneous administration • 2 significant findings: Melanotan I tolerable and effective at : • melanin density in the skin (significant) • UV-induced sunburn cells (significant) in subjects most at risk for UV induced skin damage • 1% increase in melanin density => skin cancers roughly decreases by a factor of 2 MTI beneficial as a protection against UV-induced skin damage in populations most at risk for sunlight-induced skin damage and carcinogenesis Phase III, 1991
Melanotan I Ac-Ser-Tyr-Ser-Met-Glu-His-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH2 • Melanotropins : the minimal message sequence (bioassays in frog and lizard skin) α-MSH : minimal sequencerequired for agonisticactivity, minimal chainlength for observable biologicalactivity Important potentiating AA, contibutesignificantly to the biopotency of alpha MSH A super potentmelanotropin????? How??? • Protectα-MSH from inactivation by oxidativemechanisms : Ac-Ser-Tyr-Ser-Met-Glu-His-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH2 Norleucine : resulting analogue active or more active in most bioassays D-enantiomerinstead of L-Phe : analoqueproved to be 10-1000 times more active in one or more bio essays
Melanotan II • Lactam bridgebetweenaminoacids5 and 10 • Subcutaneous administration • Much more activethanMelanotan I in stimulatingmelanogenesis • Verylong t1/2 Ac -Nle- Asp-His-D-Phe-Arg-Trp-Lys-NH2
Melanotan I and II • Advantages of those peptides : • Capacity of increasingmelanin production => of skin cancer incidence Photoprotectivestrategy: «tanningwithout the sun»