Download
1 / 53
540 likes | 700 Views
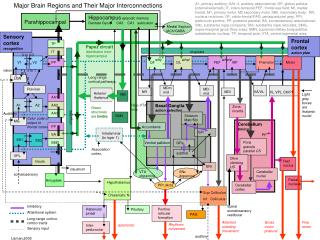
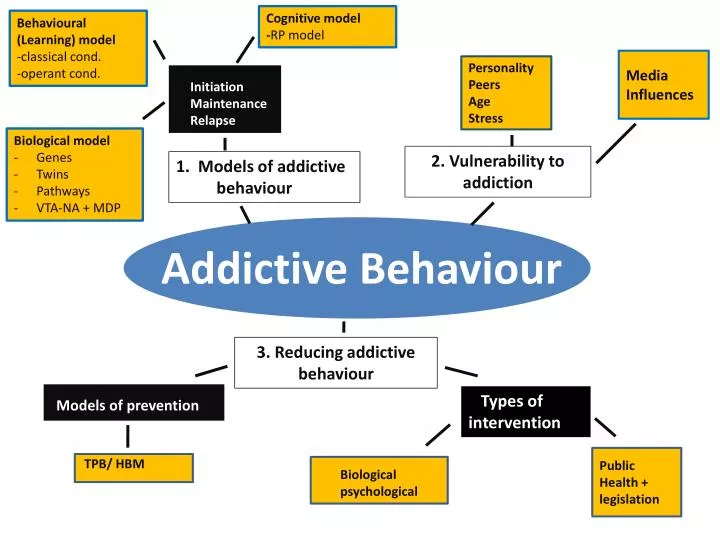
Cognitive model - RP model. Behavioural (Learning) model -classical cond. -operant cond. Media Influences. Personality Peers Age Stress. Initiation Maintenance Relapse. Biological model Genes Twins Pathways VTA-NA + MDP. 2. Vulnerability to addiction .

E N D
Cognitive model -RP model Behavioural (Learning) model -classical cond. -operant cond. Media Influences Personality Peers Age Stress Initiation Maintenance Relapse • Biological model • Genes • Twins • Pathways • VTA-NA + MDP 2. Vulnerability to addiction 1. Models of addictive behaviour Addictive Behaviour 3. Reducing addictive behaviour Models of prevention Types of intervention Public Health + legislation TPB/ HBM Biological psychological
Types of intervention • Biological • Psychological • Public Health
Group Activity • Prezi Biological interventions – drugs for smoking + gambling • Millionaire Public Health interventions + Advertising campaigns • Powerpoint Psychological interventions - CBT 4. Poster Psychological interventions - Aversion therapy
Types of intervention • Biological • Psychological • Public Health
Because addiction causes so much personal distress and can create social problems such as crime and poverty, psychologists have tried to find effective ways to intervene in the cycle of addictive behaviour. • Some of these are biological (drug treatments) and others involve psychological interventions (counselling and cognitive therapy). • In this final part on addictive behaviour we examine the effectiveness of such intervention, as well as the impact of legislation in changing addictive behaviour.
Definitions • A therapy is used in psychological interventions • A treatment is used in biological interventions
DRUGS- Gambling • Hollander et al (2000) evaluated the effectiveness of fluvoxamine - a specific serotonin reuptake inhibitor (SSRI) which increases serotonin levels), in a study involving 15 people. • They were first treated with a placebo drug before entering an eight-week period of active treatment. • Although only ten people completed the study, the drug showed a significant benefit, with greater reduction in gambling and urges to gamble than in the placebo treatment phase. Acting on the re-uptake of the neurotransmitter Serotonin in the brain
Administration of naltrexone(a dopamine receptor antagonist which reduces dopamine levels), works by reducing the rewarding and reinforcing properties of gambling behaviour, thus reducing the urge to gamble.
Evaluation of Hollander et al study Low external validity (A03) • There are methodological problems with this study. It had a very small sample size (N=10) and was of a short duration (16 weeks). Low reliability (A03) • A larger and longer study (Blanco et al 2002) involving 32 gamblers over six months, failed to demonstrate any superiority for SSRI treatment over a placebo. Support • Support for the effectiveness of naltrexone comes from a study that found significant decreases in gambling thoughts and behaviours after six weeks of treatment (Kim and Grant, 2001)
Drugs - Heroine addiction • Methadone is a synthetic drug widely used in the treatment of heroin addiction. Methadone mimics the effects of heroin but is less addictive. Like heroin, it produces feelings of euphoria, but to a lesser degree, initially a drug abuser is prescribed slowly increasing amounts of methadone to decrease tolerance to the drug. The dose is then slowly decreased until the addict no longer needs either methadone or heroin. Watch video • A ‘stepped approach’ is adopted, i.e. where the • addict is gradually given less and less of the drug
Do nicotine substitutes work? • A biological treatment for reducing a smoker’s craving for nicotine is to provide it in a different way such as gum, patches or inhalers. • These are designed to help smokers endure the nicotine withdrawal that accompanies any effort to quite smoking. • However, although nicotine replacement removes withdrawal symptoms, the severity of withdrawal is only minimally related to success in stopping smoking (this means that other factors such as social and peer influences must play an important role in quitting smoking). • This, therefore, casts doubt on the logic of using nicotine replacement to help people stop (Davison et al 2004)
Activity: Nicotine substitutes - using A2 textbooks p.437 take notes Absorbed more slowly than tobacco Ex-smokers become dependant Doses delivering nicotine equivalent of one cigarette per hour causes cardiovascular changes However Prolonged use is less of of health risk than continued smoking Best results when combined with behavioural treatment Deliver nicotine slowly into bloodstream & to brain – through skin Only one patch daily Compliance easier Treatment 10-12weeks However If smoking continues while worn smoker risks increasing body nicotine to dangerous levels Newest replacement Smoker inhales through plastic tube like cigarette holder – resembles Smoking activity However Davison et al (2004) Study comparing inhalers with placebo inhalers 12 month abstinence rates – 28 percent treatment group 18 percent placebo group
Activity -Interviews Do patches/inhalers/gum work? • In pairs -construct standardised questions • Go out into the college – find smokers – and ask them about their experiences with these methods. • Report back to the class.
Uses • CBT • Aversion therapy • Advertising campaigns
Interventions based on Cognitive-behavioural Therapies (CBT) • CBT is the idea that addictive behaviours are maintained by the person’s thoughts about their behaviours. • The main goal of CBT is to help people change the way they think about their addiction, and to learn new ways of coping more effectively with the circumstances that led to these behaviours in the past (e.g. coping with difficult situations or when exposed to peer pressure). • In gambling addiction, cognitive errors such as the belief that the individual can control and predict outcomes, plays a key part in the maintenance of gambling. CBT attempts to correct these errors in thinking, thus reducing the urge to gamble.
Features of CBT • CBT attempts to correct • the errors in thinking, that the • individual can control and predict • outcomes thus reducing the urge • to gamble. Addictive behaviours are maintained by the person’s thoughts about their behaviours. • To help people change the way • they think about their addiction, and to • learn new ways of coping more effectively • with the circumstances that led to these • behaviours in the past.
Steps in CBT • 1) Teaching people to identify the physical signs of addiction (eg: tensing of the muscles, increased heart rate). Identifying the stressor to try and deal with it. • 2) Reconstructing stressful situations is an attempt to make a more realistic assessment of different addictive behaviours. Gives insight into current coping strategies • 3) Compensation through self-improvement Insights gained can be used to move forward and learn new techniques of dealing with stress ie: seeing addictive behaviours as challenges.
Interventions based on Cognitive Models (social cognition and health models) TPB Model • According to this model, the effectiveness of strategies aimed at modifying health behaviour, depends on the success in influencing the persons intention to engage in the specific behaviour. Since behaviour is determined by intentions, a change in behavioural intention should produce a change in the associated behaviour. The behavioural and normative beliefs (which underlie the attitudes towards the behaviour and relevant subjective norms respectively) should be the target of the interventions (Stroebe, 2000). • When designing a campaign to influence behaviour we need to consider whether to focus on behavioural or normative beliefs. This decision will depend on the relative importance of the beliefs and norms in determining the behaviour in question. The relative importance will also vary between different populations, so it is important to conduct pilot studies when designing and intervention.
Activity: A2 textbook (p. 434-435) complete the following; Ladouceur et al’s (2001) study on gambling.... Gamblers reported positive results by using CBT.. • Procedure • Two groups of p’s, 1=CBT 2= None • Results • 54% of participants in CBT group improved by 50% compared with 7% of control group • 85% of treatment group compared with • 14% of control group achieved 50% improvements on three of four measures used • (e.gfrequency of gambling, control over gambling behaviour) • Maintained at 6, 12 and 24 month follow up • Other researchers on smoking • Cognitive researchers encouraged smokers to have more ‘control’ by helping them develop coping skills (e.g. relaxation, positive talk) in tempting situations such as after a meal) • However... • Davisionet al (2004) suggests overall “Results are not promising”
Smoking.. • Smoking as an example: Although smokers generally acknowledge the harmful effects of smoking, information about these effects is unlikely to persuade smokers to quite. (Leventhal& Cleary 1980). Similarly the perceived threat of contracting HIV has been found to have only a small association with condom use among heterosexuals (Sheeran et al 1999). Interventions that focus on the dangers of HIV and AIDS are, therefore, unlikely to be effective in increasing condom use. • According to this model, it should be possible to change attitudes towards health damaging behaviours by modifying the environment (increase the price of cigarettes and alcohol, restrictions on their sale). However, the costs must be sufficiently high to outweigh the rewards.
The Health Belief Model According to HBM, interventions are most likely to induce people to adopt some precautionary behaviour if; a) they can be persuaded that they are susceptible to some disease, b) developing that disease will have serious consequences, • adopting the preventative behaviour will make them less susceptible or reduce the severity of the disease, and the perceived benefits will outweigh the anticipated costs Strobe (2000) cites a study of 300 sexually active Scottish teenagers, which investigated the relationship between the various components of the HBM and the intention to carry and use condoms.
Perceived severity of HIV infection, perceived vulnerability to infection and perceived effectiveness of condom use were only weakly related to intention. However, perceived barriers to condom use (such as belief about pleasure reduction, awkwardness of using a condom and partners’ likely response to suggested use) were significantly related to intentions to carry and use condoms. • These findings suggest that instead of emphasising vulnerability to infection, the severity of infection and condom effectiveness; future interventions might prove more effective by focusing on social acceptability barriers.
Interventions based on Classical Conditioning (Learning model) Aversion Therapy • In aversion therapy, some undesirable response to a particular stimulus is removed by associating the stimulus with another, aversive stimulus. += • For example, alcohol is paired with an emetic drug (which induces severe nausea and vomiting), so the nausea and vomiting become a conditioned response to alcohol.
Aversion therapy clip An example ……
Activity …How would you explain how this works .. Using the scientific terms…
In pairs - Fill in the gaps .. UCS UCR + UCS UCR NS Smoking CR CS
Interventions based on Classical conditioning Aversion Therapy An undesirable response to a particular stimulus is removed by associating the stimulus with another, aversive stimulus Emetic drug Nausea/Vomiting UCS UCR Emetic drug + Smoking UCS Nausea/Vomiting UCR NS Nausea/Vomiting Smoking CR CS
Research Evidence on the use of Aversion Therapy Meyer and Chesser (1970) Half alcoholic patients abstained for one year following treatment better than having no treatment Roth and Fonagy (2005) – Studies used electric shocks in random control trials. Results across trials inconsistent - only a short term impact with this technique Smith et al (1997, in Roth and Fonagy) Matched 249 patients in multimodel treatment (chemicals or electric aversion) Similar number of controls (from programme that used counselling) Aversion therapy group - higher rates of abstinence at 6 mthsnot sustained at 12 mth Covert sensitisation - a variant of aversion therapy Behaviour to be removed and aversive stimulus are imagined Patient visualises events leading to start of undersirable behaviour as it happens imagine nausea of some aversive sensation ‘Sensitization achieved by associating undesirable behaviour with disagreeable result Aversion therapy & Gambling (McConagh et al 1983, in Bennett 2006) Compared aversion therapy with imagined sensitization Latter proved most effective on measures of gambling urge and behaviour over year following treatment
Outcomes of therapies Covert sensitization has proved the most effective therapy on measures of gambling urge and behaviour over the year following treatment. Long-term follow-up, conducted between two and nine ears after the end of therapy, found that 79 per cent of those who took part in the desensitisation programme reported control over or having stopped gambling. Just over 50 per cent of the aversion therapy group reported the same outcome.
Public Health Interventions (PHI)and Legislation • According to Ogden (2004) public health interventions aim to promote behaviour change in whole populations (all individuals, not just those seeking help) and have been increasingly popular in recent years. In the case of smoking cessation, such interventions take the form of:
Doctor’s advice • Worksite interventions • Community-wide approaches • Government interventions
EVALUATION Activity: Complete PFC of the Russell et al 1979 smoking study (page 438) of A2 textbook Procedure: Smokers allocated to one of four groups: • follow up only • questionnaire about smoking behaviour and follow up • doctor’s advice to stop smoking, questionnaire about smoking + follow up • doctor’s advice to stop smoking, leaflet giving advice and follow up All participants followed up at one and 12 months Findings: Percentages of those in all groups still not smoking were 0.3, 1.6, 3.3 and 5.1 respectively Although small, if all GPs recommended giving up – 500,000 less smokers in a year Conclusion: Effectiveness of doctor’s advice increased if trained in patient-centred counselling techniques (Rogers 1951- client/person-centred therapy in Gross 2005)
Smoking Interventions Types of worksite Interventions • No smoking policies • Work-based health promotion programmes • Voluntary until July 2007 • Now all enclosed public places and workplaces in England are smoke-free Benefits • Reach many who would not attend hospital or clinic • Large numbers increase group motivation and social support • Eliminates danger of secondary passive smoking
Research into worksite interventions • Conflicting results. Some studies report overall reduction in number of cigarettes smoked for up to 12 months. • Some smoking outside work compensates for reduced work smoking (Ogden 2004) • Two Australian studies – public sector workers following bans in 4 office buildings • Survey attitudes after felt inconvenienced but improved 6 months later.Only 2% gave up completely.
Aim of community based programmes • For those who won’t attend clinics • Used for group motivation & social support • Part of drive to reduce coronary heart disease Research into community based Programmes Standard Five City Project (Farquhar et Al 1990) • Experimental group -Intensive face-to-face instruction re how to Stop smoking • Exposed to media Info on how to quit. Results - 13% reduction rate compared to controls. North Karelia Project (Puska et al 1985) • Target community had Intensive educational campaign compared to those in • Neighbouring community not in campaign. Results - 10% reduction in men compared to controlsand 24% reduction in Cardiovascular deaths.
Form of Government Interventions • Restricting/banning advertising of cigarettes in 2003 • Alcohol adverts governed by legislation and self-regulation, i.e. to show alcohol it must not be seen to improve social or sexual success or make the drinker popular or more attractive. • Discouraging dangerous behaviour e.g. Drinking at work or when driving Research into Government Interventions • Research indicates a relationship between cost of cigs and alcohol and their consumption (Ogden 2002). • Increasing price could promote smoking and drinking cessation and discourage people starting – especially young children • Health Models can contribute to perceived costs of behaviour (for treating illnesses) and perceived benefits of behaviour change
clips • Smoking • Smoking • quit
Class timed exam question.. “Describe two forms of public health interventions together with research evidence.” (10 marks)
“Critically consider two or more types of intervention for addictive behaviour, including their effectiveness in dealing with initiation and /or relapse “ ( 8 + 16 marks) • No plan!!