Download

1 / 17
170 likes | 392 Views
HEPARIN PLUS ALTEPLASE COMPARED WITH HEPARIN ALONE IN PATIENTS WITH SUBMASSIVE PULMONARY EMBOLISM. KONSTANTINIDES N Engl J Med, Vol. 347, No. 15 · October 10, 2002 Arnold SEVERAC DES Pneumologie Montpellier . INTRODUCTION.

E N D
HEPARIN PLUS ALTEPLASE COMPARED WITH HEPARIN ALONE IN PATIENTSWITH SUBMASSIVE PULMONARY EMBOLISM KONSTANTINIDES N Engl J Med, Vol. 347, No. 15· October 10, 2002 Arnold SEVERAC DES Pneumologie Montpellier
INTRODUCTION • L’utilisation des thrombolytiques dans l’embolie pulmonaire est controversée. • Recommandée en cas d’instabilité hémodynamique ou choc. Dalen JE, Alpert JS, Hirsch J. Thrombolytic therapy for pulmonary embolism : is it effective? Is it safe? When is it indicated? Arch Intern Med1997;157:2550-6. • Intérêt chez les patients hémodynamiquement stable débattu. Goldhaber SZ. Thrombolysis in pulmonary embolism: a debatable indication.Thromb Haemost 2001;86:444-51. Konstantinides S, Geibel A, Kasper W. Submassive and massive pulmonaryembolism: a target for thrombolytic therapy? Thromb Haemost 1999;82:Suppl 1:104-8.4. Goldhaber SZ. Thrombolysis
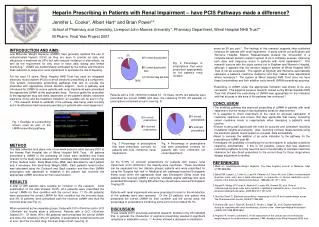
INTRODUCTION • Étude randomisée, prospective, contre placebo, multicentrique (47 centres). • Héparine (5000 U + 1000 UI\h) vs Héparine + Actilyse (10 mg puis 90 mg sur 2 h). • Uniquement chez les patients ayant une embolie pulmonaire sub-massive. • HTAP. • Dysfonction ventriculaire droite. • Instabilité hémodynamique exclusion
256 patients enrôlés 118 dans groupe actilyse, 138 dans groupe placebo. Caractéristiques similaires dans les deux groupes.
CONCLUSION • Traitement par actilyse associé à héparinothérapie : • Améliore l'évolution clinique des patients avec moins de nécessité d'escalade thérapeutique. • Est un traitement sûr • Peut être recommandé pour les embolies pulmonaires sub-massives.
DISCUSSION • Traitement interessant mais ne diminu en fait que la nessécité de recourir à une thrombolyse ultérieure.
DISCUSSION • Traitement interessant mais ne diminu en fait que la nessécité de recourir à une thrombolyse ultérieure. • Pas de surmortalité retrouvé dans cette étude mais peut etre différent en dehors d'une étude clinique : • Contre-indication. • Surveillance.
DISCUSSION • Une étude rétrospective de 128 patients. • Dans le groupe thrombolyse : 15,6% d'accidents hémorragiques et 6,25% de décés contre 0% dans le groupe héparine. Hamel E, Pacouret G, Vincentelli D, et al. Thrombolysis or heparin therapy in massive pulmonary embolism with right ventricular dilation:results from a 128-patient monocenter registry. Chest 2001;120:120-5. • Une autre étude retrouve 1,9% d'hémorrhagie cérébrale après thrombolyse. Kanter DS, Mikkola KM, Patel SR, Parker JA, Goldhaber SZ. Thrombolytic therapy for pulmonary embolism: frequency of intracranial hemorrhage and associated risk factors. Chest 1997;111:1241-5.
CONCLUSION • La thrombolyse peut avoir un intérêt dans l'embolie pulmonaire sub-massive. • Traitement non dénué de risque. • Impératif de respecter les contre-indications. • Possibilité de réserver ce traitement en secours en cas de mauvaise évolution car pas de différence de mortalité entre les deux attitudes.