Ventilator Classification
Ventilator Classification. 215a. Classification of Mechanical Ventilation. Kacmarek’s “ 12 Point Classification “ •Positive/Negative Pressure •Powering Mechanism •Driving Mechanism •Single or Double Circuited •Modes of Ventilation •Cycling Parameter.

Ventilator Classification
E N D
Presentation Transcript
Classification of MechanicalVentilation • Kacmarek’s “ 12 Point Classification “ •Positive/Negative Pressure •Powering Mechanism •Driving Mechanism •Single or Double Circuited •Modes of Ventilation •Cycling Parameter
Classification of MechanicalVentilation •Limits •Flow Patterns •Pressure Patterns •Internal Resistance •Auxiliary Maneuvers •Alarms
Classification of MechanicalVentilation • Positive or Negative Pressure • Most Ventilators are positive pressure • Not physiological • May cause “side effects” of PPV • Above ambient pressure created at mouth • Intra-alveolar pressure is ambient • Creating a positive intrapulmonary pressure
Classification of MechanicalVentilation • Negative Pressure • Physiological • Pressure gradient atmospheric to subatmospheric • No Intubation needed • Difficult to work with patient • Usually used at home or rehab. • Less control over patient settings/parameters • Examples; Iron Lung & Chest Cuirass
Powering Mechanism -Electric • Only delivers 21% without addition of O2 • Uses high pressure oxygen for FiO2 over 21% • MA1 • Need electrical generator for power outages Used in patients without need for supplemental O2, O2 can be used by attaching a Oxygen tubing and infusing it to the circuit Home care patients---RARE
Powering Mechanism -Pneumatic • Plugged into high pressure gas source • Uses 2 gas sources air and oxygen at 50 psi • Uses reducing valves to lower pressure • Pneumatic only applies to machines that are only powered by gas such as IPPB machines (Birds)
Powering Mechanism -Combined • Both pneumatically and electronically controlled • Applies to most ventilators used in the hospital setting • Examples: • Puritan Bennette 7200, 840 • Servo 900C, I • Hamilton Galileo • Drager
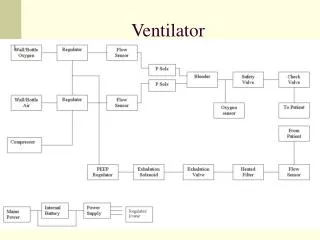
Driving Mechanism • Pneumatics • Clutch & Valve = Bennett PR • Servo = Siemens, Servo and Baby Bird • Solenoids = Bourns Bear, BP200 • Regulator = Bourns Bear, BP200 • Fluidics = Monoghan225, Ohio550 • Piston (NOT USED ANY LONGER) • Linear = Bourns,LS104-150,Gill 1 • Rotary = Morch, Emerson, Engstrom
Single or Double Circuited • • Single Circuit A single circuit is one in which the gas supply that powers the ventilator is the same gas that is delivered to the patient • Examples = PB 840, Servo I HAS NOTHING TO DO WITH ACTUAL CIRCUIT
Single or Double Circuited • • Double Circuit A double circuit has a gas source that powers the unit by compressing a bag or bellows containing the gas that will go to the patient • Examples = MA1,Monohan USED IN ANESTHSIA BUT NOT IN MODERN VENTS
Modes of Ventilation • Control Mode The Ventilator is responsible for the initiation and delivery of each tidal volume. The Ventilator sets both rate and volume no spontaneous breaths delivered. Ventilator does all the work of breathing for patient. Vents now days are not entirely controlled…
Modes of Ventilation • Assist The patient is totally responsible for initiation of the inspiratory phase, but the ventilator delivers the volume. Patient totally sets rate
Modes of Ventilation • Assist/Control Patient is allowed to trigger a breath. If a patient fails to trigger a breath the controlled breath will cycle on per time. The assisted breath is completed by the machine, the patient will always get the preset volume or pressure, they can however contribute more than the set volume, but not pressure.
SIMV • Patient can breathe spontaneously from the • ventilator via a demand valve, ventilator • has a preset rate in which it functions in the • control mode and delivers that rate to the • patient at a set volume. The rate is synchronized • with patient assist preventing stacking of breaths.
MMV • A minimum minute volume is set on the ventilator. • The patient may receive this volume by, spontaneous breaths, by being mechanically ventilated or a combination of both if spontaneous minute volume falls below set amount ventilator would make up difference. • Not commonly used, Old Servos and Dragers
PSV • The patient’s inspiratory effort is assisted by the • ventilator which functions as a constant pressure • generator up to a preset level of pressure or • until inspiratory flow rates decrease to 25% of peak • flow. This mode can only be used with modes • that allow spont. breaths & volumes. Ex SIMV, • Independently or CPAP mode • Used to overcome RAW and increase spontaneous VT
Types and modes of mechanical ventilation • A confusing assortment of possible ways to mechanically ventilate a patient’s lungs is available to the clinician, and these ways are distinguished by numerous variables. Phase variables are used to initiate one of the three phases (trigger, limit, and cycle) of the ventilatory cycle. • The trigger variable, which causes inspiration to begin, can be a preset pressure variation (pressure triggering), a preset volume (volume triggering), a designated flow change (flow triggering), or an elapsed time (time triggering). • The limit variable is the pressure, volume, or flow target that cannot be exceeded during inspiration. An inspiration may thus be limited when a preset peak airway pressure is reached (pressure limiting), when a preset volume is delivered (volume limiting), or when a preset peak flow is attained (flow limiting). • Cycling refers to the factors that terminate inspiration. A breath may be pressure, volume, or time cycled when a preset pressure, volume, or flow as time interval has been reached, respectively.
Cycling Parameter’s • All ventilation is a function of flow, time, pressure or volume • Cycling is what ends inspiration and starts exhalation • Volume, Pressure or Time can end inspiration • What ever ends inspiration and starts exhalation determines the type of ventilator. ( note a ventilator may have more then one cycling parameter)
Limits • Any other than normal cycling are limits • Example: When a pressure limit is set on a volume ventilator it will not allow the ventilator to exceed that limit even though the volume has not been delivered, the ventilator would cycle into expiratory phase Pressure limit set in pressure control. Most vents have pressure “pop offs”. Volume limit set in Volume control
Flow Pattern • Square Wave or Rectangular = constant flow, depending on internal resistance to determine if it changes with back pressure • Decaying or Descending = reaches peak flow immediately, then gradually decelerates
Flow Patterns • Sine or Sinusoidal = gradually increasing flow until mid-inspiration, due to action of rotary piston. Best distribution of gas. • Accelerating or Ascending = gradually accelerates to peak and then levels off • NO LONGER USED
Pressure Patterns • Pressure is determined by flow pattern Rectilinear = due to square wave Sigmoidal = due to sine wave Exponential = due to accelerating Parabolic = due to decaying
PEEP, Inspiratory hold, Sigh • PEEP = positive pressure remains in the lungs at all times to keep open alveoli • Inspiratory Hold = better distribution of gas throughout lung fields, best V/Q match, used to achieve a platue pressure/static pressure for static compliance • Sigh = for prevention of atelectasis, simulate normal breathing, 1.5 times set Vt (RARE) • Expiratory Retard = simulates pursed lip breathing
Goals and Objectives for Invasive Mechanical Ventilation • To replace in whole or in part the normal functions of the lungs and ventilatory pump in patients whose ability to maintain these functions is temporarily or permanently impaired • To provide these functions with as little disruption of homeostasis and with as few complications as possible
Physiologic objectives • To improve alveolar ventilation, as indicated by arterial PCO2 and pH • To improve arterial oxygenation, as indicated by arterial PO2, saturation, and/or oxygen content • To increase end-inspiratory lung inflation • To increase end-expiratory lung volume (functional residual capacity) • To reduce the work of breathing (i.e. to unload the ventilatory muscles)
Clinical objectives • To reverse acute respiratory acidosis: to relieve immediately life-threatening acidemia, rather than necessarily to make arterial PCO2 and/or pH normal • • To reverse hypoxemia: to increase arterial PO2 (generally such that arterial saturation is 90% or more, e.g. to ≥ 60 mm Hg), in order to reverse or prevent clinically important tissue hypoxia • To relieve respiratory distress: to relieve patient discomfort while the primary disease process resolves or improves • To prevent or reverse atelectasis: to avoid or correct adverse consequences of incomplete lung inflation • To reverse ventilatory muscle fatigue: to unload the ventilatory muscles and allow them to rest while the causes of increased work load are reversed or improved
Clinical objectives • To permit sedation and/or neuromuscular blockade: to allow the patient to be rendered unable to breathe spontaneously, as during surgery or certain ICU procedures • To decrease systemic or myocardial oxygen consumption: in certain settings (e.g. severe ARDS; cardiogenic shock), when spontaneous breathing or other muscular activity impairs systemic or cardiac oxygenation • To reduce intracranial pressure, by means of controlled hyperventilation, as in acute closed head injury • To stabilize the chest wall, as in chest wall resection or massive flail chest
Indications for Mechanical Ventilation • Apnea and Impending Respiratory Arrest • No one would argue with providing ventilatory support for a patient who has stopped breathing altogether. On the other hand, "impending respiratory arrest" is difficult to define prospectively, and attempts to study it as an indication for intubation and mechanical ventilation have so far proved unsuccessful. These things are commonly carried out because the clinician judges the patient to be in severe respiratory distress, "tiring," or "about to arrest," but inter-observer variation and the extent to which these subjective impressions predict an unfavorable outcome if intubation is not performed have not been investigated.
Indications for Mechanical Ventilation • Exacerbation of Chronic Obstructive Pulmonary Disease • Invasive mechanical ventilation is used when patients with acute exacerbations of COPD have cardiovascular instability, somnolence or other altered mental state, uncooperativeness, a high risk of aspiration, copious or very viscous respiratory tract secretions, any craniofacial condition (such as recent trauma or surgery) potentially rendering NPPV difficult, or extreme obesity. Very severe or progressive respiratory acidosis is also accepted as an indication, but agreement is lacking as to whether a pH of 7.25, a PaCO2 of 60 mm Hg, or some other thresholds should be used.
Indications for Mechanical Ventilation • Acute Severe Asthma • Retrospective studies have shown that relatively few patients with acute severe asthma require invasive mechanical ventilation, but no clinical trials to define the specific indications have been reported. These indications may be similar to those for acute COPD exacerbations, although the potential for more rapid physiologic improvement in asthma, and the fact that patients with asthma are typically younger and healthier than those with severe COPD raise doubt about this assumption. Unlike the situation with COPD exacerbations, the benefit of NPPV in acute severe asthma has not yet been clearly established
Indications for Mechanical Ventilation • Neuromuscular Disease • In acute respiratory insufficiency complicating neuromuscular disorders such as the Guillain-Barré syndrome and myasthenia gravis, there is agreement among experienced clinicians that invasive mechanical ventilation is best initiated before the patient develops frank respiratory acidosis. Vital capacity and the maximum inspiratory pressure generated against an occluded airway have been used in assessing the need for intubation in such patients
Indications for Mechanical Ventilation • Acute Hypoxemic Respiratory Failure • Severe hypoxemia by itself is seldom an indication for invasive mechanical ventilation. For example, isolated hypoxemia in patients who have diffuse pneumonia or pulmonary edema can often be managed with high-flow oxygen by mask, with or without continuous positive airway pressure (CPAP). Typically, patients who demonstrate severe hypoxemia in the setting of severe acute illness have other indications for ventilatory support, such as evidence for excessive work of breathing or diminished ventilatory drive. There is no evidence to indicate what threshold of PaCO2/FIO2 or other measure of oxygenation failure should be used as an independent indication for intubation and mechanical ventilation, or in fact whether such a threshold exists.
Indications for Mechanical Ventilation • Heart Failure and Cardiogenic Shock • Available evidence on the management of cardiac pulmonary edema indicates that CPAP or NPPV may improve gas exchange--possibly with a reduced need for intubation--but that rates of clinical recovery and other outcomes may not be different compared to management without these interventions. Cardiogenic shock, however, may represent a separate indication for invasive mechanical ventilation, to decrease the oxygen cost of breathing at a time of severely impaired cardiac function. While this has not been subjected to a prospective clinical trial, retrospective studies of patients managed with intra-aortic balloon pumps have found higher rates of weaning from the pump and improved hospital mortality in patients who were intubated and ventilated.
Indications for Mechanical Ventilation • Acute Brain Injury • Short-term hyperventilation can rapidly decrease intracranial pressure in patients with traumatic brain injury by constricting cerebral blood vessels and decreasing both cerebral blood flow and cerebral blood volume. However, available evidence indicates that routine hyperventilation in such patients does not improve survival or neurologic outcome, and may in fact worsen the latter. Although brief periods of hyperventilation are used acutely to reduce sudden increases in intracranial pressure while more definitive measures are undertaken, the presence of acute brain injury is not by itself an indication for hyperventilation.
Alarms • Alarms • Oxygen Disconnect • High/Low Pressure • High/Low Volume • Fail to Cycle • High/Low PEEP • Time ( I:E Ratio ) • Apnea