Download
1 / 18
220 likes | 573 Views
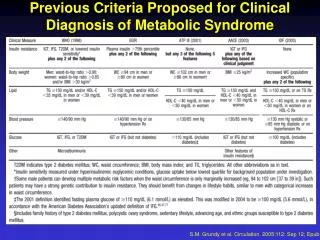
FPG. 2-Hour PG on OGTT. Diabetes Mellitus. Diabetes Mellitus. 126 mg/dL. 7.0 mmol/L. 200 mg/dL. 11.1. mmol/L. Impaired Fasting. Impaired Glucose. Glucose. Tolerance. 110 mg/dL. 6.1 mmol/L. 140 mg/dL. 7.8. mmol/L. Normal. Normal. Criteria for Diagnosis of DM. **.

E N D
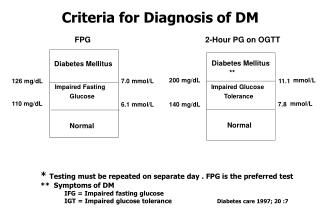
FPG 2-Hour PG on OGTT Diabetes Mellitus Diabetes Mellitus 126 mg/dL 7.0 mmol/L 200 mg/dL 11.1 mmol/L Impaired Fasting Impaired Glucose Glucose Tolerance 110 mg/dL 6.1 mmol/L 140 mg/dL 7.8 mmol/L Normal Normal Criteria for Diagnosis of DM ** * Testing must be repeated on separate day . FPG is the preferred test ** Symptoms of DM IFG = Impaired fasting glucose IGT = Impaired glucose tolerance Diabetes care 1997; 20 :7
Overview of Type 2: Screening and Diagnosis Patient w. Risk Factors and/or Symptoms of Diabetes May screen using capillary blood: FCG>110 mg/dL (6.1 mmol/L) or CCG>160 mg/dL (8.9 mmol/L) then proceed to diagnostic test Fasting Plasma Glucose (FPG) or Casual Plasma Glucose (CPG) FPG 110-125 mg/dL (6.1 - 6.9 mmol/L) CPG 140-199 mg/dL (7.8 - 11.0 mmol/L) FPG > 126 mg/dL (7.0 mmol/L) CPG> 200 mg/dL (11.1 mmol/L) FPG < 110 mg/dL (6.1 mmol/L) CPG< 140 mg/dL (7.8 mmol/L) Repeat FPG within 7 days If only FPG criteria then: Impaired Fasting Glucose If CPG criteria then: Impaired Glucose Homeostasis Diagnosis of Diabetes if FPG > 126 mg/dL (7.0 mmol/L) Type 1 or Type 2 Diabetes dependent upon age and ketones No Diabetes
High-risk groups : screening 1. Age > 45 yrs if normal check 3 yrs interval 2. Age < 45 yrs with 2.1 Obesity (BMI > 27 kg/m2) 2.2 First degree relatives 2.3 Hypertension (>140/90 mmHg.) 2.4 Dyslipidemia (HDL-cholesterol < 35 mg/dl. and/or triglyceride >250 mg/dl.) 2.5 Gestational DM or macrosomia ( > 4 kg.) 2.6 previous impaired glucose tolerance(IGT) or impaired fasting glucose (IFG) 2.7 Habitual physical inactivity 2.8 polycystic ovary syndrome ADA ,Diacetes care 2001.
Overview of Type 2: Screening and Diagnosis Patient w. Risk Factors and/or Symptoms of Diabetes May screen using capillary blood: FCG>110 mg/dL (6.1 mmol/L) or CCG>160 mg/dL (8.9 mmol/L) then proceed to diagnostic test Fasting Plasma Glucose (FPG) or Casual Plasma Glucose (CPG) FPG 110-125 mg/dL (6.1 - 6.9 mmol/L) CPG 140-199 mg/dL (7.8 - 11.0 mmol/L) FPG > 126 mg/dL (7.0 mmol/L) CPG> 200 mg/dL (11.1 mmol/L) FPG < 110 mg/dL (6.1 mmol/L) CPG< 140 mg/dL (7.8 mmol/L) Repeat FPG within 7 days If only FPG criteria then: Impaired Fasting Glucose If CPG criteria then: Impaired Glucose Homeostasis Diagnosis of Diabetes if FPG > 126 mg/dL (7.0 mmol/L) Type 1 or Type 2 Diabetes dependent upon age and ketones No Diabetes
หลักการพิจารณาการรักษาผู้ป่วยเบาหวานหลักการพิจารณาการรักษาผู้ป่วยเบาหวาน At Diagnosis Fasting plasma glucose < 200 mg/dL Casual plasma glucose < 250 mg/dL Medical Nutrition Therapy And Exercise ( within 3 months) At Diagnosis Fasting plasma glucose 200-350 mg/dL Casual plasma glucose 250-400 mg/dL Oral Hypoglycemic Agent BMI < 25 BMI > 25 Metformin Sulfonylurea target not reach in 4-8 wk Target control FPG 80-140 mg/dL 2 hr PP PG < 160 mg/dL HbA1c < 7% Combination Different group of oral drugs (Awareness of side effect)
Combination Different group of oral drugs (Awareness of side effect) At Diagnosis Fasting plasma glucose > 350 mg/dL Casual plasma glucose > 400 mg/dL Combination of Oral Agent + Bedtime Insulin (intermediate or long acting) : insulin stage 1 target not reach in 4-8 wk Insulin stage 2 + insulin enhancer (BID Regimen) R/N-0-R/N-0, LP/N-0-LP/N target not reach in 4-8 wk Insulin stage 3A : (R/N-0-R/N, LP/N-0-LP-N) Insulin stage 3A-Mid : (R-R-R/N-0, LP-LP-LP/n-0) Target control FPG 80-140 mg/dL 2 hr PP PG < 160 mg/dL HbA1c < 7% target not reach in 4-8 wk Insulin stage 4A : (R-R-R-N, LP-LP-LP-N)
Choosing the “Best” Therapy--Type 2First Step: Major Contraindications for Oral Agents Liver function and serum creatinine No liver disease select Thiazolidinedione Liver disease select insulin yes Serum creatinine > 2 mg/dL no yes Serum creatinine 1.4-2 mg/dL Metformin contraindicated No liver disease consider other oral agents Liver disease select insulin no Serum creatinine <1.4 mg/dL *Since oral agents pass through the placental barrier they should be avoided in pregnancy. Oral agents have not been tested in individuals <18 years of age.
Oral Agent - Monotherapy Sulfonylurea Lean patient Initial Rx-early in disease Use with caution in renal disease Metformin Obese, insulin resistant Dyslipidemia Cr <1.5 First Line Rx ? Thiazolidinediones Insulin resistant Inappropriate for metformin Can use in renal insufficiency Troglitazone not advised as MonoRx Acarbose Post meal hyperglycemia No hypoglycemia Limited potency Repaglinide Post-meal hyperglycemia Variable schedule Alternative to SU May use in renal insufficiency Alternate Rx
Insulin Therapy in Type 2 Diabetes Insulin Sensitizer + Bedtime Insulin Metformin + Bedtime NPH Thiazolidinedione + Bedtime NPH ( Metformin or TZD) + SU + Bedtime NPH Sulfonylurea + Bedtime NPH (limited benefit) Insulin Therapy Two daily injections R/N - 0 - R/N - 0 LP/N - 0 - LP/N - 0 Two Daily injections + Insulin Sensitizer Stage 2 Three daily injections R/N - 0 - R - N LP/N - 0 - LP - N Three daily injections + Insulin Sensitizer Stage 3 Four daily injections R/(N) - R - R - N LP/(N) - LP - LP - N LP/U - LP - LP/U - (LP) LP/U - LP - LP - N Four daily injections + Insulin Sensitizer Stage 4
Hypertension: Diagnosis and Treatment Initiation Blood Pressure Evaluationat Every Office Visit No Diagnosis of HTN BP>130/85 (2X) Repeat Every Visit Yes Initiate ACE inhibitor Yes Microalbuminuria No Systolic BP >140 or Diastolic BP >90 No Food Plan and Activity Follow-up 1-2 months Yes Initiate Drug Therapy Staged Diabetes Management
Dyslipidemia: Diagnosis and Treatment Initiation Annual Fractionated Lipid Profile No Diagnosis of Dyslipidemia Repeat Screening in 1 year Yes Fibric Acid Yes Tg > 1000 mg/dl No LDL Cholesterol Elevated? LDL > 100 with CVD LDL > 130 without CVD No Food Plan and Activity Follow-up 1-2 months Yes Statin Staged Diabetes Management
Risk Profile Diabetes + Known CVD Diabetes + High Risk Diabetes + Lower Risk Initiate Rx LDL > 100 (statin) LDL > 130 (statin) LDL > 130 (MNT) Treatment Decisions LDL Cholesterol in Adults with Diabetes Target LDL < 100 LDL < 100 LDL < 100 Staged Diabetes Management Institute for Clinical Systems Integration Adapted from American Diabetes Association. Diabetes Care 21 (Suppl 1):S36, 1998.
Retinopathy: Screening and Diagnosis Complete Eye Examination No Evidence of Retinal Lesion Repeat Annually Yes ENPDR: microaneurysms, dot hemorrhages, hard exudates NPDR: microvascular abnormalities, severe dot hemorrhages, venous dilation PDR: new vessels on disc, retinal detachment Tight glycemic control HbA1c <7 % Refer to Eye Specialist within 1-3 Months Immediate Referral to Eye Specialist Staged Diabetes Management
SDM Algorithm for Screening, Diagnosis of Microalbuminuria Obtain annual random urine sample (first Am urine preferred) Repeat screen annually If hypertension present consider ACEI or other Rx NO Test positive? YES Repeat screen twice within 60 days, R/O occult UTI, exercise
SDM Algorithm for Screening, Diagnosis of Microalbuminuria (continued) NO Repeat screen annually 2 of 3 tests positive? YES Diagnosis of microalbuminuria Initiate ACE inhibitor
Definitions of Abnormalities in Albumin Excretion Random** 24 hr Urine Timed (microgram/min) Normal <30 mg/g <30 mg/24h <20 Microalbuminuria 30-300 mg/g 30-300 mg/24h 20-200 Macroalbuminuria >300 mg/g >300 mg/24h >200 ** Random urine = Alb/Cr ratio Diabetes Care 28, Supple 1, Jan 1998
Prevention & Treatment of Nephropathy • Tight glucose control • Low protein diet • Tight blood pressure control • ( < 130/85 mmHg ) • ACE Inhibitors (Low dose) • Cessation of smoking • Treatment of dyslipidemia
Diabetic Foot: Assessment and Treatment Complete Foot Examination: deformities, sensation, ulcers, circulation, ischemia Yes Assess and Treat : measurements, surgical debridement, antibiotics, vascular evaluations Evidence of Ulcer No Normal foot Abnormal foot: deformity, insensate, ischemia Foot assessment each visit, self-care Special foot wear, palliative foot care, self-care Staged Diabetes Management