Effects of Tenofovir/FTC on Vitamin D, Calcium, and Parathyroid Hormone Levels in HIV Patients
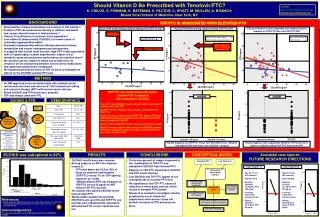
This study evaluates the impact of Tenofovir (TDF) and Emtricitabine (FTC) on vitamin D status and calcium metabolism in HIV-infected individuals. We found that patients on TDF/FTC exhibited higher plasma parathyroid hormone (PTH) levels, particularly those with suboptimal 25(OH)D levels. This suggests that vitamin D deficiency, related to TDF/FTC use, contributes to hyperparathyroidism and impacts bone health. Our findings highlight the necessity for routine monitoring of vitamin D and PTH levels in HIV patients on TDF/FTC therapy to prevent bone mineral density loss.

Effects of Tenofovir/FTC on Vitamin D, Calcium, and Parathyroid Hormone Levels in HIV Patients
E N D
Presentation Transcript
Tenofovir/FTC Low Vitamin D 50 200 200 Decreased Whole-body Calcium 40 150 150 PTH pg/ml 30 PTH pg/ml Percentage Kidney Damage (Fanconi-like Syndrome) 20 100 100 Decreased Bone Mineral Density Increased PTH 10 Increased Excretion of Phosphate 50 50 200 0 Increased Resorbption of Calcium Increased Excretion of Phosphate 200 <10 10-20 20-30 30-40 40-50 50-60 60-70 >70 25(OH)D ng/ml Deficient 0 0 Non-TDF/FTC ART TDF/FTC ART Before After Before After Suboptimal 200 Low Serum Phosphate Optimal Excessive p=0.045 150 150 150 PTHpg/ml PTH pg/ml 100 100 100 50 50 50 0 0 0 0 10 20 30 40 50 60 0 10 20 30 40 50 60 25(OH)D < 30 ng/ml 25(OH)D > 30 ng/ml 25(OH)D ng/ml 25(OH)D ng/ml TDF/FTC was associated with higher plasma PTH in subjects with suboptimal 25(OH)D 200 p=0.021 Fig 1) PTH and 25(OH)D levels among subjects taking ART not including TDF/FTC Fig 2a) PTH and 25(OH)D levels among subjects taking TDF/FTC Fig 2b)Among subjects taking TDF/FTC, plasma PTH was significantly higher in subjects with suboptimal 25(OH)D than with optimal 25(OH)D Fig 3a) PTH and 25(OH)D levels among all subjects on ART Fig 3b) Among subjects with suboptimal 25(OH)D, plasma PTH was significantly higher in subjects taking TDF/FTC than those on other ART. Low Vitamin D 150 Decreased Serum Calcium PTHpg/ml 100 Increased Parathyroid Hormone 50 Supply Calcium at Cost to Bone 0 TDF/FTC ART NOT TDF/FTC Case Report 1) Case Report 2) • Age 53, 17 yrs HIV infection • TDF/FTC/EFZ • Baseline 25(OH)D 10.3ng/ml, PTH 159 pg/ml • 5 months VitaminD3/ Calcium citrate • Repeat 25(OH)D 24.5ng/ml, PTH 85 pg/ml • Age 55, 20 yrs HIV infection • TDF/FTC/EFZ • Baseline 25(OH)D 15.1ng/ml, PTH 139 pg/ml • 3 months VitaminD3/ Calcium citrate • Repeat 25(OH)D 35.4 ng/ml, PTH 78 pg/ml ShouldVitamin D Be Prescribed with Tenofovir/FTC?K. CHILDS, S. FISHMAN, K. BATEMAN, S. FACTOR, C. WYATT, M. MULLEN, A. BRANCH; Mount Sinai School of Medicine, New York, NY. Contact: kathryn.childs@mssm.edu or andrea.branch@mssm.edu BACKGROUND TDF/FTC IS ASSOCIATED WITH ELEVATED PTH TDF/FTC IS ASSOCIATED WITH ELEVATED PTH • Abnormalities of bone and calcium are common in HIV patients.1 • Tenofovir (TDF) decreases bone density in children and adults and causes skeletal lesions in fetal primates.2,3 • Vitamin D insufficiency is common in the population4 • Low vitamin D [measured by25(OH)D] is a known cause of secondary hyperparathyroidism • Secondary hyperparathyroidism indicates abnormal calcium metabolism and causes osteopenia and osteoporosis. • In subjects with normal renal function, high PTH is also associated with LV hypertrophy, incident hypertension, higher risk of metabolic syndrome and poorer performance on cognitive tests5,6 • We aimed to assess vitamin D status and to determine its influence on the relationship between anti-retroviral medications and abnormal calcium/bone metabolism. • We hypothesized that the effect of TDF on bone is mediated via effects on the 25(OH)D-calcium-PTH axis Fig 2a) PTH levels among subjects taking TDF/FTC ART Fig 3a) PTH level is more dependant on 25(OH)D level in subjects on TDF/FTC than non-TDF/FTC ART Fig 1) PTH levels among subjects taking non-TDF/FTC ART Lower Limit Optimal 25(OH)D 200 TDF/FTC ART, low 25(OH)D TDF/FTC ART, optimal 25(OH)D Non-TDF/FTC ART Many subjects on TDF/FTC had PTH above the ULN 150 PTH Upper Limit Normal PTH pg/ml 100 50 METHOD • An IRB approved cross-sectional study with medical record review and interviews was done on 51 HIV-infected men taking anti-retroviral therapy (ART) with normal serum calcium. • Blood 25(OH)D and PTH levels were assayed. • TDF was always used with FTC. 0 0 10 20 30 40 50 60 25(OH)D ng/ml 25(OH)D & PTH DEMOGRAPHICS PTHpg/ml Secondary Hyperparathyroidism Osteoporosis Bone pain Muscle weakness Fatigue Cardiovascular disease Immunological impairments Fig 2b) Subjects on TDF/FTC: Those with 25(OH)D levels <30ng/ml had higherPTH than those with 25(OH)D >30ng/ml Fig 3b) Subjects with suboptimal 25(OH)D:PTH levels were higher in subjectstaking TDF/FTC than other ART a For continous variables, value is median (interquartile range) 25(OH)D was suboptimal in 82% RESULTS CONCLUSIONS CONCEPTUAL MODEL Anecdotal case reports: FUTURE RESEARCH DIRECTIONS • 25(OH)D insufficiency was common • Among subjects on ART who had low vitamin D: • PTH was above the ULN in 39% of those on tenofovir/emtricitabine (TDF/FTC) versus 7% on TDF-sparing regimens (p= 0.036) • Median plasma PTH was 80 pg/ml on TDF/FTC versus 55 pg/ml on ART without TDF/FTC (p=0.02). • No subject with optimal 25(OH)D levels had elevated PTH • Multivariable analysis showed that 25(OH)D levels (p=0.03) and TDF/FTC use (p=0.04) were independently associated with plasma PTH, serum creatinine was not. • Thirty-nine percent of subjects exposed to the combination of TDF/FTC and suboptimal 25(OH)D had elevated PTH • Patients on TDF/FTC should have 25(OH)D and PTH levels checked • Low 25(OH)D and TDF/FTC appear to act synergistically to increase PTH level • We hypothesize that TDF/FTC causes a reduction in whole body calcium, which results in elevated PTH (model) • Research is needed to investigate whether prophylactic use of vitamin D3 supplements and calcium citrate will prevent increases in PTH and preserve • bone. • References • Brown and Qaqish AIDS 2006 2) Purdy et al J.Pediatr 2008 3) Gallant et al JAMA 2004 4) Holick MF. N Engl J Med 2007 5)Saleh et al. Eur Heart J 2003 6) Forman et al Hypertension 2008. • Acknowledgements • The work was supported, in part, by NIH grants DA016156 and DK066939 • (to ADB)