Download
1 / 32
320 likes | 458 Views
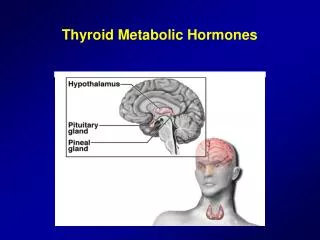
Thyroid hormones in health and disease. Dr S Razvi Endocrinologist and Senior Lecturer 1 st October 2013. Agenda. Physiology Clinical data and evidence Some real life cases – interactive Summary. Hypothalamus. TRH. TSH. TSH. Thyroid Gland. T 4. T 3. T 4 è T 3

E N D
Thyroid hormones in health and disease Dr S Razvi Endocrinologist and Senior Lecturer 1st October 2013
Agenda • Physiology • Clinical data and evidence • Some real life cases – interactive • Summary
Hypothalamus TRH TSH TSH Thyroid Gland T4 T3 T4è T3 Liver, Muscle Hypothalamic-Pituitary-Thyroid AxisClinical Utility • TSH reflects tissue thyroid hormone actions • TSH for diagnosis of hypothyroidism and thyrotoxicosis • TSH as an index of therapeutic success and potential toxicity Pituitary T4 T3 Adapted from Merck Manual of Medical Information. ed. R Berkow. 704:1997.
Individual vs population reference range (e.g., serum TSH) A B 2.5th 0.4 mU/L 97.5th 4.0 mU/L
Factors affecting thyroid function (TSH) • Age • Gender • Smoking • Iodine status • Illness • Pregnancy
Effect of age Surks & Hollowell, 2007
Raised TSH • Cholesterol increases with TSH • Associated with heart disease in younger (<65/70 yr olds) • Higher risk of progression to overt hypothyroidism (particularly if TPO +ve) • Associated with heart failure
Leiden 85+ study Gussekloo et al, JAMA 2004
Low TSH • Associated with atrial fibrillation • Osteoporosis • Higher cardiovascular mortality (only if TSH undetectable <0.1 mU/L) • Dementia
Consequences of Mild Hypothyroidism Fetal Brain Development • Children of women with untreated hypothyroidism during pregnancy: • Averaged 7 points lower on IQ testing* • Had a significant percentage (19%) of IQ 85 IQ Scores of 85 Children of Mothers with Untreated Hypothyroidism 19% (P<0.005) Control Children 5% 0 5 10 15 20 25 *Full-scale Wechsler Intelligence Scale for Children. Haddow JE, et al. N Engl J Med. 1999;341:549-555.
Guidelines for raised TSH • If TSH > 10 consistently then treat. • For consistently raised TSH in younger people (70 – 75 yrs) with symptoms – a trial of treatment is recommended for 3 – 6 months. • For consistently raised TSH in older people (> 75 yrs) – wait and watch policy. • Pregnancy: should be treated with aim for low normal TSH
Guidelines for low TSH • If TSH consistently < 0.1 (suppressed) AND if other risk factors (AF, osteoporosis) or symptoms – treat. • If TSH mildly low and asymptomatic - wait and watch policy. • In pregancy, low TSH is of no consequece (normal in 1st trimester).
Case 1 • 45 year old woman • Seen by GP for tiredness • Examination and all other Ix normal • TSH 6.6 mIU/L (0.4 – 4.0) • FT4 15.6 pmol/L (9 – 22) • TPO positive • What is the diagnosis? • Is treatment beneficial?
Case 2 • 86 yr old man with forgetfulness • TSH 7.4 mU/L FT4 15.4 pmol/L • Treat?
Case 3 • 34 yr old lady trying to conceive • TSH 5.4 mU/L FT4 12 pmol/L • Treat?
Case 4 • 32 yr old lady with weight loss, palpitations and tremor. • TSH<0.01 mU/L, FT4 42 pmol/L • Next step?
Case 4 cont • Tc uptake thyroid scan – 0% uptake • TSH receptor and TPO antibody – negative • Diagnosis? • Thyroiditis • TSH 3.5 mU/L four months later.
Case 5 • 20 yr old lady • 8/40 pregnant. On LT4 100 mcg/day • What would you do next? Check TFTs Possibly increase LT4 to 125 mcg/day Refer her to antenatal endocrine clinic
Case 6 • 68 yr old woman presents with • Next step? TFT, TPO Refer to endocrinology / ENT USS +/- FNA (3-5% cancer)
Case 7 • 34 yr old man on LT4 (150 mcg/day) after thyroidectomy for Graves’ disease • TSH 13.5 mU/L FT4 12.6 pmol/L • Next step? Intermittent compliance (mainly)
How Common Is Suboptimal Thyroxine Therapy? 30% 20% 10% Excessive Thyroxine Therapy 22% 21% 18% 14% Inadequate Thyroxine Therapy 15% 10% 20% 30% 18% 18% 27% Ross, 1990 Hollowell, 2002 Canaris, 2000 Parle, 1993 32% 48% 40% 33% Ross DS, et al. JCEM.1990;71:764-769. Parle JV, et al. Br J Gen Pract. 1993;43:107-109. Canaris GJ, et al. Arch Intern Med. 2000;160:526-534. Hollowell J, et al. JCEM. 2002;87:489-499.
Conditions and medications affecting thyroid function (including those on LT4) • Iron • Calcium • PPI • Coeliac disease • Pernicious anaemia • Amiodarone • Lithium Consider taking LT4 at a different time prior to increasing the dose Different formulations may have varying strengths
Take home messages • Thyroid function is affected by multiple processes. • Slightly high TSH in elderly may not have an adverse impact. • In pregnancy, high TSH should always be treated. • Overt hyperthyroidism should always be referred to endocrinologists for further assessment. • Thyroid nodules need specialist assessment with USS and ?FNA