Download
1 / 93
930 likes | 1.3k Views
Revascularisation in Renal artery stenosis. Dr Bijilesh u. Atherosclerosis accounts for about 90% of cases of renal artery stenosis in people over age 40 Fibromuscular dysplasia - the other major cause.

E N D
Revascularisation in Renal artery stenosis Dr Bijilesh u
Atherosclerosis accounts for about 90% of cases of renal artery stenosis in people over age 40 • Fibromuscular dysplasia - the other major cause
Percutaneous intervention has become very popular for treating atherosclerotic renal artery stenosis • use of stents has boosted the rate of technical success • more cases are being discovered incidentally during angiography of other arteries
Number of angioplasty-stenting procedures performed every year is on the rise • Yet there is no overwhelming evidence that intervention yields clinical benefits—ie, better blood pressure control or renal function— than does medical therapy
RENAL INTERVENTIONS ON THE RISE • Renal angioplasty began replacing surgical revascularization in the 1990s • Less-invasive , more readily available, similar clinical outcomes • Last decade, stent placement during angioplasty has become standard - improving the rates of technical success
HOW COMMON IS RENAL ARTERY STENOSIS • Prevalence of RAS depends on the definition used and the population screened. • More common in older patients who have risk factors for other vascular diseases than in the general population • Affect between 1% and 5% of patients with hypertension • Derkx FH, Schalekamp MA. Renal artery stenosis and hypertension. Lancet. 1994; 344: 237–239 • Renal artery stenosis is found in 11% to 28% of patients undergoing diagnostic cardiac catheterization • White CJ, Olin JW .Diagnosis and management of atherosclerotic renal artery stenosis: improving patient selection and outcomes. Nat ClinPractCardiovasc Med 2009; 6:176–190.
No studies of the prevalence of renal artery stenosis have been performed in the general population • Holley et al in an autopsy series, found renal artery stenosis of greater than 50% in 27% of patients over age 50 and in 56.4% of hypertensive patients • Prevalence was 10% in normotensive patients
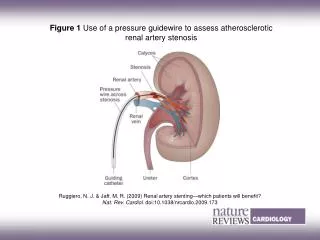
Renal Doppler ultrasonography can detect stenosis only if the artery is narrowed by more than 60% • Hansen et alused ultrasonography to screen 870 people over age 65 and found a lesion (a narrowing of more than 60%) in 6.8%. • Angiography can detect less-severe stenosis define RAS as a narrowing > 50% severe disease - narrowing > 70% • Unilateral stenosis needs to be more than 70% to pose a risk to the kidney • Cohen MG, et al. A simple prediction rule for significant renal artery stenosis in patients undergoing cardiac catheterization. Am Heart J 2005; 150:1204–1211
WHO IS AT RISK? Factors associated with a higher risk of finding RAS on a radiographic study • Older age , Female sex • Hypertension , Three-vessel CAD • Peripheral artery disease • Chronic kidney disease • Diabetes , Tobacco use • Low HDL • Cohen MG, et al. A simple prediction rule for significant renal artery stenosis in patients undergoing cardiac catheterization. Am Heart J 2005; 150:1204–1211
HOW OFTEN DOES STENOSIS PROGRESS • In studies that used duplex ultrasonography, roughly half of lesions smaller than 60% grew to greater than 60% over 3 years • Risk of total occlusion of an artery was relatively low and depended on the severity of stenosis: 0.7% if the baseline stenosis was less than 60% and 2.3% to 7% if it was greater • Caps MT, Perissinotto C, Zierler RE, et al . Prospective study of atherosclerotic disease progression in the renal artery. Circulation 1998; 98:2866–2872
Schreiber and colleagues _ compared serial angiograms obtained a mean of 52 months apart in 85 patients who did not undergo intervention • Stenosis had progressed in 37 (44%), and to the point of total occlusion in 14 (16%) • Schreiber MJ, Pohl MA, Novick AC .The natural history of atherosclerotic and fibrous renal artery disease • 1998 study found progression in 11.1% over 2.6 years • Crowley JJ, et al.Progression of renal artery stenosis in patients undergoing cardiac catheterization
Rates of progression differed because – • Indications for screening were different (clinical suspicionvs routine screening during CAG) • Severity of stenosis at the time of diagnosis- different • Fewer people were taking statins.
FOUR CLINICAL PRESENTATIONS OF RENAL ARTERY STENOSIS • Clinically silent stenosis • Renovascular hypertension • Ischemic nephropathy • Recurrent “flash” pulmonary edema
Recurrent “flash” pulmonary edema • Less common presentation • Occurring in patients with critical bilateral renal artery stenosis or unilateral stenosis in an artery supplying a solitary functioning kidney • Most have severe hypertension (average systolic blood pressure 174–207 mm Hg) and poor renal function
Association between pulmonary edema and bilateral renal artery stenosis was first noted in 1998 by Pickering et al • Several case series showed that 82% to 92% of patients with recurrent pulmonary edema and renal artery stenosis had bilateral stenosis • Pickering TG, et al. Recurrent pulmonary oedema in hypertension due to bilateral renal artery stenosis: treatment by angioplasty or surgical revascularisation. Lancet 1988; 2:551–552 • Later case series corroborated this finding: 85% to 100% of patients with renal artery stenosis and pulmonary edema had bilateral stenosis • Messina LM, Zelenock GB, Yao KA, Stanley JC. Renal revascularization for recurrent pulmonary edema in patients with poorly controlled hypertension and renal insufficiency: a distinct subgroup of patients with arteriosclerotic renal artery occlusive disease. J VascSurg 1992; 15:73–80 • Gray BH, et al. Clinical benefit of renal artery angioplasty with stenting for the control of recurrent and refractory congestive heart failure. Vasc Med 2002; 7:275–279.
STENTING IS NOW STANDARD • Stenting has become standard in the endovascular treatment of renal artery stenosis • Most atherosclerotic renal artery lesions are located in the ostium and many are extensions of calcified aortic plaque • Textor SC. Ischemic nephropathy: where are we now? J Am Soc Nephrol 2004; 15:1974–1982 • These hard lesions tend to rebound to their original shape more often with balloon angioplasty alone • Stenting provides the additional force needed to permanently disrupt the lesion- longer-lasting result
Rates of technical success are higher with stents than without them (98% vs 46%– 77%) • Beutler JJ, et al. Long-term effects of arterial stenting on kidney function for patients with ostial atherosclerotic renal artery stenosis and renal insufficiency. J Am Soc Nephrol 2001; 12:1475–1481 • If the lesion is ostial, this difference is even more impressive (75% vs 29%) • Restenosis rates at 6 months are lower with stents (14% vs 26%–48%) • Van de Ven PJ, et al. Arterial stenting and balloon angioplasty in ostial atherosclerotic renovascular disease: a randomized trial. Lancet 1999; 353:282–286
GOALS: LOWER THE BLOOD PRESSURE, SAVE THE KIDNEY • Endovascular procedures pose some risk to the patient -critical to intervene only in patients most likely to respond clinically • In renovascular HTN - improve blood pressure control • In ischemic nephropathy- slow the decline in renal function or to improve it
Commonly cited indications for intervention in renal artery stenosis
Stenting may not improve renal function • Coincidental RAS in a patient with unrelated CKD is very hard to differentiate from true ischemic nephropathy • Most patients with ischemic nephropathy do not benefit from revascularization, making it challenging to identify those few whose renal function may respond
In a prospective cohort study in 304 patients with CKD & RAS who underwent surgical revascularization, Textor reported that serum creatinine improved - in 28% worsened in 19.7% remained unchanged in 160 - 52.6% • Textor SC. Revascularization in atherosclerotic renal artery disease. Kidney Int 1998; 53:799–811
Davies et alfound that 20% of patients who underwent renal stenting had a persistent increase in serum creatinine of 0.5 mg/dL or more • Nearly three times more likely (19% vs 7%) to eventually require dialysis • Lower 5-year survival rate (41% vs 71%) • Davies MG, et al. Implications of acute functional injury following percutaneous renal artery intervention. Ann VascSurg 2008; 22:783–789
Zeller et alfound that renal function improved slightly in 52% of patients who received stents • Mean decrease in serum creatinine in this group was 0.22 mg/Dl • However, the other 48% had a mean increase in serum creatinine of 1.1 mg/dL .Zeller T, et al. Predictors of improved renal function after percutaneous stent-supported angioplasty of severe atherosclerotic ostial renal artery stenosis. Circulation 2003; 108;2244–2249.
Stenting usually improves flash pulmonary edema • Acute pulmonary edema in the setting of bilateral RAS - improvement in clinical status can be expected in most patients after intervention • Blood pressure improves in 94% to 100% • Messina LM, Zelenock GB, Yao KA, Stanley JC. Renal revascularization for recurrent pulmonary edema in patients with poorly controlled hypertension and renal insufficiency: a distinct subgroup of patients with arteriosclerotic renal artery occlusive disease. J VascSurg 1992; 15:73–80 • Renal function either improves or stabilizes in 77% to 91% • Pulmonary edema resolves without recurrence in 77% to 100% • Gray BH, et al. Clinical benefit of renal artery angioplasty with stenting for the control of recurrent and refractory congestive heart failure. Vasc Med 2002; 7:275–279.
Major randomized trials • Scottish and Newcastle Renal Artery Stenosis Collaborative Group • EssaiMulticentrique Medicaments vsAngioplastie (EMMA) Study Group • Dutch Renal Artery Stenosis Intervention Cooperative (DRASTIC) study • STAR TRIAL • ASTRAL TRIAL • CORAL TRIAL
Before stents came into use, several randomized controlled trials found that blood pressure was no better controlled after angioplasty except in cases of bilateral stenosis • This may be because stenosis tended to recur after angioplasty without stents
Scottish and Newcastle Renal Artery Stenosis Collaborative Group study • Randomised comparison of percutaneous angioplasty vs continued medical therapy for hypertensive patients with atheromatous renal artery stenosis • Methods • Out of 135 eligible patients 55 (44%) were randomised • Eligible patients had sustained hypertension, with a minimum diastolic BP of 95 mm Hg on at least two anti-hypertensive drugs • RAS was defined by renal angiography as at least 50% stenosis in the affected vessel
Scottish and Newcastle Renal Artery Stenosis Collaborative Group Results: • BP fell in angioplasty and medical groups • Bilateral RAS - a statistically significant (P < 0.05) fall in bp • Mean fall in bp - 26/10 mm hg • In unilateral RAS, no statistically significant differences in outcome were observed • No significant differences or trends in serum creatinine were observed between the two groups • Major outcome events (death, MI , heart failure, stroke, dialysis) were similar
Scottish and Newcastle Renal Artery Stenosis Collaborative Group Conclusions • In hypertensive patients with atheromatous RAS percutaneous renal angioplasty results in a modest improvement in systolic BP compared with medical therapy alone • This benefit was confined to patients with bilateral disease. • No patient was 'cured', renal function did not improve, and intervention was accompanied by a significant complication rate. • J Webster, F Marshall, M Abdalla, A Dominiczak, R Edwards, C G Isles, H Loose, J Main, P Padfield, I T Russell, B Walker, M Watson and R Wilkinson on behalf of the Scottish and Newcastle Renal Artery Stenosis Collaborative Group J Hum Hypertens 1998; 12:329–335
Blood Pressure Outcome of Angioplasty in Atherosclerotic Renal Artery StenosisEssaiMulticentrique Medicaments vsAngioplastie (EMMA) Study Group • Aim - document the efficacy and safety of angioplasty for lowering BP in patients with atherosclerotic RAS • Randomly assigned to antihypertensive drug treatment (control group, n=26) or angioplasty (n=23) • Primary end point - 24 hour ambulatory BP - measured at baseline and at termination(6 months after randomization) • Secondary end points were the incidence of complications
EMMA • Early termination was required for refractory hypertension in 7 patients in the control group. • Antihypertensive treatment was resumed in 17 patients in the angioplasty group • Mean ambulatory BP at termination did not differ between control (141±15/84±11 mm Hg) and angioplasty (140±15/81±9 mm Hg) groups • Two patients in the control group and 6 in the angioplasty group suffered procedural complications (RR 3.4; 95% confidence interval, 0.8 to 15.1)
Angioplasty allowed easier BP control than medication alone • Antihypertensive agents - required at termination for all control patients but not for 6 of the 23 allocated to angioplasty (26%) • Moreover, 7 of 25 patients in the control group (28%) developed refractory hypertension leading to secondary angioplasty within 6 Months
Conclusion EMMA • Angioplasty madeBP control easier in the short term but was more frequently associated with complications than conservative management in patients with unilateral atherosclerotic RAS • Plouin PF, Chatellier G, Darne B, Raynaud A Blood pressure outcome of angioplasty in atherosclerotic renal artery stenosis: a randomized trial. EssaiMulticentrique Medicaments vsAngioplastie (EMMA) Study Group. Hypertension 1998; 31:823–829.
Draw backs EMMA • Only unilateral renal artery disease was enrolled • Groups were not well balanced - 23 patients for angioplasty and 26 for control • Cross-over - seven of the control-group crossed over to intervention group • High complication rate in angioplasty group which was about (6 of 23, or 26%)
Dutch Renal Artery Stenosis Intervention Cooperative (DRASTIC) study • Examined the effect of angioplasty on BP control in RAS • Overall, intervention (balloon angioplasty without stents in 54 of 56 patients, with stents in the other 2) carried no benefit • However, in subgroup analysis, the patients who crossed over because of resistant hypertension were more likely to benefit from angioplasty • van Jaarsveld BC, et al.The effect of balloon angioplasty on hypertension in atherosclerotic renal-artery stenosis. Dutch Renal Artery Stenosis Intervention Cooperative Study Group. N Engl J Med 2000; 342:1007–1014
Randomly assigned 106 patients with HTN who had atherosclerotic RAS (luminal diameter < 50 %) and a serum creatinine 2.3 mg/dl or less to undergo PTRA or to receive drug therapy • Also had to have a diastolic BP > 95 mm Hg or higher despite treatment with two antihypertensive drugs • Blood pressure, doses of antihypertensive drugs, and renal function were assessed at 3 and 12 months, and patency of the renal artery was assessed at 12 months
CONCLUSION • No significant differences between the angioplasty and drug-therapy groups in systolic and diastolic blood pressures, daily drug doses, or renal function • In the treatment of patients with hypertension and renal-artery stenosis, angioplasty has little advantage over antihypertensive-drug therapy
LIMITATIONS • Sample size was not sufficient to detect a significant difference between treatment groups • Renal artery stenosis was defined as greater than 50% stenosis • High rate of cross over - Twenty-two of 50 patients randomized to medical therapy crossed over to the angioplasty group
Operative vs interventional treatment for renal artery ostial occlusive disease (RAOOD) • 50 patients (female 18, male 32, mean age 64.4 years) with RAOOD of at least 70% stenosis in one or both renal arteries • Randomized to either OSRP (n = 25 patients, 49 arteries) or PTRA + stent (n = 25 patients, 28 arteries)
Patients were followed on a regular basis for 4 years and longer • Endpoints were re-occurrence of RAOOD and impairment of either kidney function or RVH
Results • Directly procedure-related morbidity was 13% in the interventional group and 4% in the surgical group • Four-year follow-up mortality was 18% vs 25% • Both groups showed significant improvement of RVH (P < .001) as well as improvement or stabilization of renal function • Both treatment modalities showed good early results concerning RVH, kidney function, and renal perfusion
limitations • Single center • Groups were not well balanced (PTRA+ stent group number= 22, Surgical group = 27) • Power calculation was not mentioned
Despite the lack of evidence supporting revascularization of renal artery stenosis, many interventionalists practice under the assumption that the radiographic finding of renal artery stenosis alone is an indication for renal revascularization • Only three randomized controlled trials in the modern era attempt to examine this hypothesis: STAR, ASTRAL, and CORAL
STAR TRIALJune 2000 and December 2005 • Randomized trial - medical treatment of renal artery stenosis was compared with medical treatment plus stenting • 140 Patients with RAS and renal insufficiency were randomized to revascularization with stenting (n = 64) versus continued medical management (n = 76) • Renal artery stenosis >50% luminal narrowing • Renal insufficiency - creatinine clearance <80 ml/min/1.73 m2 • Patients could crossover from medical therapy to stent placement if necessary for refractory HTN
Study Design • Patients Screened: 185 • Patients Enrolled: 140 • Mean Follow Up: 2 years • Mean Patient Age: 66 years • Female: 33%
From: Stent Placement in Patients With Atherosclerotic Renal Artery Stenosis and Impaired Renal Function:
Hypertension was treated to <140/90 mm Hg with the use of diuretics, CCB , beta blockers • All patients received atorvastatin 10 mg & aspirin 75-100 mg daily
No difference in baseline characteristics between the groups Stent group – • Mean age was 66 years • 33% were women • mean creatinine was 1.7 mg/dl • mean systolic blood pressure was 160 mm Hg, • mean number of antihypertensive drugs was 2.8, • >90% stenosis was present in 34%.