Download
1 / 46
460 likes | 657 Views
Impact of BPH Medical Treatment on Sexual Function. Wayne J.G. Hellstrom, M.D., F.A.C.S. Professor of Urology Tulane University Health Sciences Center New Orleans, Louisiana. Goals of BPH Medical Therapy. SYMPTOM RELIEF+++ SLOW DOWN DISEASE PROGRESSION. SIDE EFFECTS QUALITY OF LIFE

E N D
Impact of BPH Medical Treatment on Sexual Function Wayne J.G. Hellstrom, M.D., F.A.C.S. Professor of Urology Tulane University Health Sciences Center New Orleans, Louisiana
Goals of BPH Medical Therapy SYMPTOM RELIEF+++ SLOW DOWN DISEASE PROGRESSION SIDE EFFECTS QUALITY OF LIFE SEXUALITY
What’s all this ED-EjD stuff all about?
AUA Guidelines • “The adverse event profile appears slightly different between the four alpha-blocking agents, e.g., tamsulosin appears to have […] a higher probability of ejaculatory dysfunction than the other alpha blockers.” • “Alfuzosin, doxazosin, tamsulosin and terazosin are appropriate treatment options for patients with LUTS secondary to BPH. Although there are slight differences in the adverse-event profiles of these agents, the Panel believes that all four agents have equal clinical effectiveness.” AUA guideline on BPH, J. Urol. 2003; 170, 530-547
AUA Meta-AnalysisIncidence of Libido Problems Estimated occurrence rate with 95% CI 1% 3% 3% 5% 2% 3% 5% 3% AUA guideline on BPH, J. Urol. 2003; 170, 530-547
AUA Meta-Analysis Erectile Dysfunction Estimated occurrence rate with 95% CI 3% 4% 4% 5% 8% 8% 10% 9% 4% AUA guideline on BPH, J. Urol. 2003; 170, 530-547
AUA Meta-AnalysisEjaculatory Dysfunction Estimated occurrence rate with 95% CI 0% 10% 1% 4% 1% 3% 7% 1% AUA guideline on BPH, J. Urol. 2003; 170, 530-547
Placebo (n=2158) Dutasteride (n=2167) Dutasteride (2 Years) – US/EuropeSexual Disorders *p versus Placebo <0.001 * * * * 4.0 7.3 2.1 4.2 0.7 2.3 2.2 0.8 Roehrborn et al. Urology 2002;60:434-441
MTOPS (4 Years) - USSexual Disorders *p<0.05 vs Placebo * * * * * * 3.3 3.6 4.5 5.1 1.4 1.6 2.4 2.5 0.8 1.1 1.8 3.1 Placebo (n=3489) Doxazosin (n=3652) Finasteride (n=3600) Combination (n=3832) McConnell et al., N Engl J Med 2003, 349, 2387-98
Abnormal Ejaculation with Alfuzosinand Tamsulosin - US Pivotal Studies Tamsulosin (3 months) Alfuzosin OD (3 months) * ns *p < 0.001 18% 20 20 15 15 Abnormal ejaculation (%) * 10 10 6% 5 5 0.6% 0.6% 0% 0% 0 0 Tam 0.4 mg Tam 0.8 mg Pbo Alf 10 mg Alf 15 mg Pbo Lepor et al. Urology 1998;51:892-900 Roehrborn et al. Urology 2001;58:953
ABEJAC Study Treatment 2 Treatment 1 Treatment 3 10-day Washout 10-day Washout 5-day treatment 5-day treatment 5-day treatment Screening Day –10 /Day –5 Tamsulosin 0.8mg OD Placebo No treatment Alfuzosin 10mg OD Double-blind cross-over study in 57 young healthy volunteerswith normal sperm and no retrograde ejaculation Hellstrom,WJG:AUA 2005
ABEJAC StudyAssessments • Ejaculate volume • Post-ejaculate sperm concentration in urine • Retrograde ejaculation defined by sperm count in urine > 5 million Hellstrom,WJG:AUA 2005
ABEJAC Study Change in ejaculate volume Change in urine sperm concentration p=ns *Tam vs Pbo, p<0.001 Tam vs Alf, p<0.001 +1.7 +0.4 +0.3 +1.4 +1.2 -2.4 * Mean ±sd value at baseline 3.4 ± 1.4 ml Mean ±sd value at baseline 48 ± 0.5 million/ml Tamsulosin 0.8mg OD Alfuzosin 10mg OD Placebo Intent to treat population Hellstrom,WJG:AUA 2005
ABEJAC Study % subjects with decrease in ejaculate volume >20% * 90% 100 Tam vs Alf, p<0.001 Tam vs Pbo, p<0.001 90% 80 60 40 21% 13% 20 0 Placebo Alf. 10mg OD Tam. 0.8mg OD Among completers (n=48) Hellstrom,WJG:AUA 2005
ABEJAC Study • Complete absence of ejaculation: • Placebo: 0% • Alfuzosin 10mg OD: 0% • Tamsulosin 0.8mg OD: 35.4% (2/17 with retrograde ejaculation) Hellstrom,WJG:AUA 2005
ABEJAC StudySummary • Nearly all volunteers (90%) receiving tamsulosin 0.8mg had reduced ejaculation (not retrograde ejaculation) and 1 of 3 had complete absence of ejaculation • Percentage of patients with reduced ejaculation with alfuzosin 10mg similar to placebo • Further research needed to elucidate mechanisms of ejaculatory dysfunction with tamsulosin
Why is Ejaculatory Dysfunction more Frequent with Tamsulosin Compared to Alfuzosin ?Possible Explanations based on the Current Knowledge of the Physiology/Pharmacology of Ejaculation
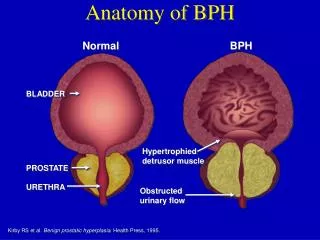
The Physiology of Ejaculation Semen volume contributions : Seminal vesicle (50-80%) Prostate (15-30%) Cowper’s gland (< 1%) Testis (< 1%) Mann and Lutwak-Mann. Male reproductive function and semen,Berlin:Springer-Verlag;1981:171-93.
The Physiology of Ejaculation Emission involves: • Secretion of seminal fluids fromthe accessory sex glands • Contractionof the seminal tractfrom the epididymis to the prostate • Closure of the bladder neck Expulsion involves : • Rythmic contractions of the striated perineal muscles (bulbospongiosus +++) & urethral smooth musculature which expel the semen
Ejaculation and Smooth Musclea1-ARs K.E. Andersson
Tamsulosin (µg/kg) Tamsulosin (µg/kg) Alfuzosin (µg/kg) Alfuzosin (µg/kg) Effects of Alfuzosin & Tamsulosinon Seminal Vesicle and Bladder Neck in Anesthetized Rat Seminal Vesicle Pressure Bladder Neck Pressure 120 120 *p <0.001 *p <0.001 * 80 80 * * * 40 40 0 0 Vehicle 3 10 3 10 Vehicle 3 10 3 10 F. Giuliano et al. BJU Int. 2004 : 93:605-8
Central Neural Control of Ejaculation K. McKenna
Spinal Ejaculation Generator Truitt and Coolen, Science 297: 1566-1569, 2002
Implication of Serotonin (5-HT) in the Central Control of Ejaculation • Pharmacological experiments • 5-HT control of ejaculation has been demonstratedpharmacologically in conscious rat using: • para-chlorophenylalanine, inhibitor of 5-HT synthesis1 • 5-hydroxytryptophan, the precursor of 5-HT2 • Increasing 5-HT level led to delayed ejaculation 1: Mitler et al., Physiol Behav, 1972, 8:1147 2: Ahlenius et al., Psychopharmacol (Berl), 1979, 65:137
140 Placebo 120 Fluvoxamine 100mg Fluoxetine 20mg 100 Paroxetine 20mg Sertraline 50mg 80 60 40 20 0 0 1 2 3 4 5 6 Daily Selective Serotonin Reuptake Inhibitor (SSRI) Treatment Delays Ejaculation Mean ejaculation latency time (seconds) Weeks Waldinger MD, Hengeveld MW, Zwinderman, AH:J.Clin.Pssychopharmacol.1998;18:274‑81.
The Key Role for 5HT1A Receptors • Activation of postsynaptic 5-HT1Areceptors by the selective 5-HT1A receptor agonist8-hydroxy-2-(di-n-propylaminotetralin) 8-OH-DPAT in male rats resultedin : • a dose dependent reduction in the number of intromissions preceding ejaculation, • a shortening of ejaculation latency. Ahlenius, S., Larsson K. Pharmacol BiochemBehav, 15: 785, 1981
8-OH-DPAT: Gold Standard of 5HT1A Agonists • 8-OH-DPAT 0,4 mg/kg : 45-55% rats ejaculate prematurely. 25-35 % of the males ejaculated extravaginally1 • At a high dose some rats ejaculate extra vaginally2 • Facilitation of the male rat ejaculatory behavior by 8-OH-DPAT is centrally mediated • Facilitation of rat ejaculatory behavior by 8-OH-DPAT fully antagonized by pretreatment with a selective 5-HT1A receptor antagonist3 Acute treatment with 8-OH-DPAT: a pharmacologically induced model of premature/rapid ejaculation in rat 1Haensel S.M. et al Pharmacol. Biochem. Behav. 1991 2Schnurr SL et al Physiol Behav 1989, 45 :897-901 3S. Br J Pharmacol. 1998;125:1733-43
Binding Data for 5HT1A Receptors by 1-Blockers Alfuzosin (IC50) Doxazosin (IC50) Tamsulosin (IC50) 5HT1A >10 µM>10 µM0.74 nM • Tamsulosin has an affinity almost equivalent to its α1A affinity for 5HT1A receptors : • KiS : 0.14 nmol/L for 1A and 0.74 for 5HT1A Receptors Andersson & Wyllie BJU Int. 2003
The Dopamine 2 Receptors (D2) Interaction Hypothesis • Effect of 8-OH-DPAT on male rat sexual behavior may be mediated through 8-OH-DPAT's activity at D2 receptors • D2 agonists facilitate ejaculation • D2 receptors in the paraventricular nucleus regulate genital responses and copulationin male rats Eaton RC et al Pharmacol Biochem Behav. 1991;39(1):177-81 Matuszewich L et al Brain Res. 1999;820(1-2):55-62 Giuliani D. et Ferrari F. Behav Neurosci. 1996;110(4):802-8
Comparative Affinity for D2 Receptors D2 - like ~10 µM0.28 nM Alfuzosin (IC50) Tamsulosin (IC50) Data on file sanofi-aventis
Pharmacological Model for Centrally-Induced Expulsion of EjaculationPreliminary Results
Example of a Representative Recording of Rythmic Bulbospongiosus Muscle Contractions Elicited by Intracerebroventricular Delivery of 8-OH-DPAT 8-OH-DPAT i.c.v. injection 20µg Blood pressure BS EMG bursts of BS contractions Giuliano et al. EAU 2005
Effect of 5-HT1A Antagonist (Way 100635) & D2 Antagonist (Raclopride) on 8-OH-DPAT Induced BS Contractions 8-OH-DPAT 20 µg icv 100% 7/9 80% D2 receptors areessential in mediating the effect of 8-OH-DPAT on BS muscle activity 5/9 60% 40% Responding rats 1/8 20% 0% + Veh + WAY (20 µg) + Raclo (40 µg) Giuliano et al. EAU 2005
Effect of Tamsulosin and Alfuzosin on 8-OH-DPAT Induced BS Contractions Mean BS EMG amplitude Area under the curve of BS EMG Alfu 10µg Alfu 10µg Saline Saline 0.4 Tamsu 1µg Tamsu 1µg 6 * 0.3 5 4 0.2 Area under the curve (V.s) 3 0.1 2 1 0.0 0 Saline Alfu 10µg Tamsu 1µg Saline Alfu 10µg Tamsu 1µg * Different from vehicle (p<0,05) Giuliano et al. EAU 2005
Preliminary Comments/ Conclusions • Differential effect of systemic injection of tamsulosin vs. alfuzosin on BS activity induced by i.c.v. delivery of 8-OH-DPAT in rats explains ejaculation disorders reported with tamsulosin • The effect of tamsulosin on ejaculation could be mediated by cerebral D2 receptors for which tamsulosin has a strong affinity Giuliano et al. EAU 2005
Overall Conclusions • There are differences both at the peripheral level and at the central level between alfuzosin and tamsulosin regarding the ejaculatory process • Animal experiments reveal differences between alfuzosin and tamsulosin regarding their effects along the seminal tract both in vivo and in vitro • The high affinity of tamsulosin for 5HT1A and D2 receptors - both play a key role in the central control of ejaculation – provide an alternative explanation for the effect of tamsulosin on ejaculation
Alfuzosin has the Lowest Impact on Sexuality…Could Alfuzosin have a Beneficial Effect on Sexuality ?
Compounds [µM] 0,0001 0,001 0,01 0,1 1 10 0 20 Sildenafil Phentolamine 40 Alfuzosin % Relaxation 60 80 100 Relaxing Effect of Alfuzosin, Phentolamine & Sildenafil on Rabbit Isolated Corpus Cavernosum Palea et al. BJU Int. 2003, 91, 873-877
7 EC50= 24µg/kg 6 5 4 Number of erections 3 EC50= 58µg/kg 2 Apomorphine + Alfuzosin 30µg/kg iv 1 Apomorphine 0 10 100 1000 Apomorphine (µg/kg sc) Alfuzosin Potentiates the Pro-Erectile Properties of Apomorphine F test on curve fitting (logistic equation; 4 parameters): EC50 statistically different; p=0.001. Mayoux E. et al. Eur. Urol. 2004, 45, 110-116
Alfuzosin 10 mg ODImprovement of Sexual Function? Dan-PSSsex 2,334 sexually active men 1-year treatment BAD *p vs D0 <0.001 * * * 2.4 1.9 1.7 1.3 2.0 0.7 GOOD °Symptom x Bother for men with the sexual symptom (DAN-PSSsex) van Moorselaar et al. BJU Int. 2005, 95, 603 - 608
Conclusions (1) • Treatment options of LUTS differ in theirimpact on erectile and ejaculatory functions: • 5-reductase inhibitors may cause erectiledysfunction, reduced ejaculation, decreasedlibido and gynecomastia • 1-blockers are associated with a low rate ofsexual dysfunction except tamsulosin- dose- dependent incidence of ejaculatory and erectile dysfunction compared with alfuzosin and placebo • Ejaculatory disorders observed with tamsulosinare not related to retrograde ejaculation
Conclusions(2) • Side effects of BPH medical treatment should be carefully discussed with patientsbefore initiating therapy