Download
1 / 29
290 likes | 468 Views
Acute Parenchymal Disease of Liver Acute Hepatitis Inflammation of liver caused by various agents Viral infections Hepatitis A Virus Hepatitis B Virus Hepatitis C Virus Hepatotrophic virus Hepatitis D Virus Hepatitis E Virus Cytomegalovirus Epstein Barr virus

E N D
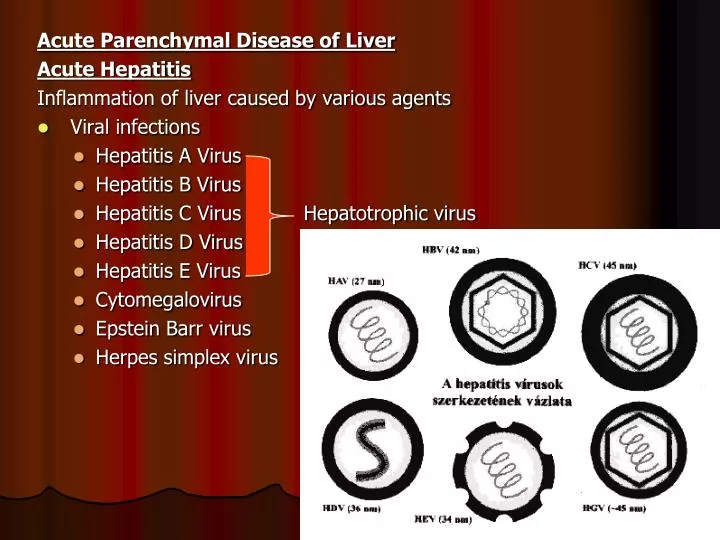
Acute Parenchymal Disease of Liver Acute Hepatitis Inflammation of liver caused by various agents • Viral infections • Hepatitis A Virus • Hepatitis B Virus • Hepatitis C Virus Hepatotrophic virus • Hepatitis D Virus • Hepatitis E Virus • Cytomegalovirus • Epstein Barr virus • Herpes simplex virus Dr S Chakradhar
Drugs – Paracetamol, Isoniazide, Rifampicin • Alcohol Others • Pregnancy • Circulatory Insufficiency • Autoimmune Hepatitis • Wilson’s Disease Viral hepatitis by hepatitis viruses which are hepatotrophic i.e. have a particular affinity for the liver Systemic viral infections involving the Liver Dr S Chakradhar
Definitions Acute viral hepatitis • is defined by the sudden onset of significant aminotransferase elevation as a consequence of diffuse necroinflammatory liver injury. Chronic viral hepatitis • is defined as the presence of persistent (at least 6 months) necroinflammatory injury that can lead to cirrhosis. • (Symptomatic, biochemical, serological & histological evidence of continuing or relapsing hepatic disease for more than 6 months) Dr S Chakradhar
HAV • Is a benign self limited, disease with an incubation period of 2 wks to 6wks. • Does not cause chronic hepatitis (5% Fulminant hepatitis) • Clinical disease tends to be mild or asymptomatic and rare after childhood • Spread by ingestion of contaminated water and food and shed in stool for 2-3 wks before and 1 week after onset of jaundice. Dr S Chakradhar
Fate of Acute Type A Hepatitis • 95% patient totally cure • 5% patient may develop Fulminant hepatitis Dr S Chakradhar
Diagnosis – Serum markers for HAV • The diagnosis of acute HAV is made by the detection of IgM anti-HAV antibody. (appears at onset of symptoms) • The recovery phase and immunity phase are characterized by IgG anti-HAV antibody. Dr S Chakradhar
HBV • HBV may be asymptomatic, acute hepatitis, chronic hepatitis & hepatocellular carcinoma • Incubation period is 1-6 months • Spread principally by transfusion of blood and blood products • Sexual contact • Vertical transmission • Use of contamination needles – drug addicts etc Dr S Chakradhar
HBV - Serum markers of HBV are: Antigens • HBsAg - Done routinely. It appears before the onset of symptoms & peaks during overt diseasein 3 – 6 months it is usually undetectable • HBcAg is not found in serum • HBeAg appears shortly after HBsAg in the serumRises early & declines rapidly Its persistence is indicative of Chronic liver disease Dr S Chakradhar
Antibodies • Anti -HBs (IgG) appears after the disappearance of HBsAg (3-6 months) and after vaccination. Persists for many years or perhaps permanently. Anti-HBs implies either a previous infection • Anti - HBcAg (IgM anti-HBc) - appears early and rapidly reaches a high titre which then subsides gradually. Anti-HBc is initially of IgM type with IgG appearing later.Suggests an acute & continuing viral replication • Anti-HBe usually indicates low-level replication and a lower degree of infectivity. Dr S Chakradhar
HCV • Is responsible for 90-95% causes of transfusion associated hepatitis. • Incubation period 2-26 wks • HCV has high rate of progression to chronic disease & eventually cirrhosis Dr S Chakradhar
HBV - Serum markers of HBV are: • Antibodies against HCV (anti-HCV) may be undetectable for the first 8 weeks after infection. • HCV RNA can be detected serum 1-3 weeks. • Positive tests are usually diagnostic in patients with elevated liver enzymes and with risk factors for the infection. • The antibody does not confer immunity. • It determines the presence of actual virus and ongoing infection. Dr S Chakradhar
HDV • It co-infects with HBV as it requires help from HBV for its replication and expression. • Mode of transmission is similar to HBV. • Incubation period – 6-9 wks Dr S Chakradhar
Diagnosis • Is made by finding HDV RNA or HDV antigen in serum or liver • And by detecting antibody to the HDV antigen. Dr S Chakradhar
HEV • Transmitted through Faecal-oral route • Does not cause chronic hepatitis • Incubation Period 3-8 weeks Dr S Chakradhar
Pathogenesis of Infective Hepatitis • Direct cytopathic effect • Induction of immune responses against viral antigen that damage virally infected hepatocytes. • Alteration of liver cell antigens and the initiation of an auto immune reaction. Dr S Chakradhar
C/F - H/O should elicit risk factors Symptoms Infection begins with a incubation period • A) Pre Icteric phase (few days to 2 wks) • Fever on and off • Anorexia, nausea, vomiting, diarrhoea • Weakness, headache, fatigue • Upper abdominal pain Dr S Chakradhar
C) Icteric phase • Jaundice • Stool become paler • Urine darker • Tenderness C) Post Icteric (Recovery phase) • Disappearance of jaundice • Urine and stool becomes normal • Appetite improves and GI symptoms subside Dr S Chakradhar
Signs • Jaundice • Tender hepatomegaly • Enlarged cervical nodes (occasionally) (Generally recovery occurs within 3-6 wks) Dr S Chakradhar
Investigations • TC, DC, ESR, Hb • LFT • Serum Bilirubin - raised • Serum Aminotransferase – Very high • Serum Alkaline Phosphatase increased • Prolonged Prothrombin time • Viral markers – Anti HAV, HBs Ag Dr S Chakradhar
Treatment • No specific treatment, only severely affected patient require hospitalization • Bed rest (till jaundice subside) • Diet – Nutrition diet (Glucose water, sugar fruit juice, soup) with slight fat restriction. • Paracetamol is preferred anti pyretic & analgesics in low doses • Avoid drugs as far as possible especially sedatives & hypnotics • Educate patient about personal Hygiene. • Vitamin B-complex Dr S Chakradhar
Complications • Chronic hepatitis • Cirrhosis of liver • Fulminant hepatic failure • Hepatic coma. • Hepatocellular Carcinoma • Bleeding Disorders Dr S Chakradhar
Prevention of Hepatitis B • Prevention depends on avoiding risk factors such as • Sharing needles • Multiple sexual partners • Blood & blood products • 2. Immunization by hepatitis B vaccine Dr S Chakradhar
Chronic Viral Hepatitis /Chronic hepatitis Classification – according to extent of inflammation • Chronic persistent hepatitis – confined to portal tract • Chronic active hepatitis – spills into the parenchyma & surrounds regions of necrotic Hepatocytes Chronic lobular hepatitis – persistent inflammation is confined to the lobule Dr S Chakradhar