Download

1 / 32
360 likes | 918 Views
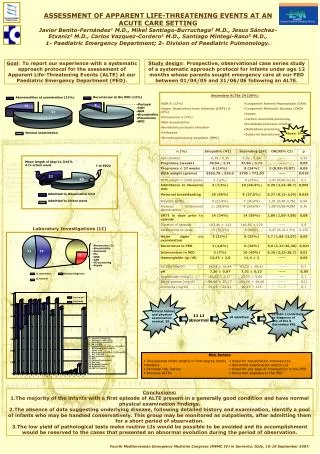
Ashna Khurana, MD Santa Clara Valley Medical Center. Apparent Life-Threatening Events (ALTE) in Infants. Goals and Objectives. Review the Differential Diagnosis for ALTE Discuss the most common Etiologies of ALTE Discuss the yield of Diagnostic Testing in infants who have had an ALTE

E N D
Ashna Khurana, MD Santa Clara Valley Medical Center Apparent Life-Threatening Events (ALTE) in Infants
Goals and Objectives • Review the Differential Diagnosis for ALTE • Discuss the most common Etiologies of ALTE • Discuss the yield of Diagnostic Testing in infants who have had an ALTE • Identify infants with ALTE that need to be Hospitalized.
Case Study • 3 week old FT female infant presents to the SCVMC ED after experiencing an episode at home where mother found the infant: • Gagging, one hour after feeding • Turned limp • Unresponsive for about 45 seconds • Cried spontaneously • Mother thinks the infant stopped breathing at the time and thought her baby was going to die.
Case Study (cont'd) • In the ED: • Stable vitals • Well appearing • Normal physical exam • ED physician pages the pediatric resident for consult and wants to know what to do with the infant.
Definition of ALTENIH Consensus Development Conference on Infantile Apnea and Home Monitoring 1986 • An episode that is frightening to the observer and is characterized by some combination: • Apnea • Color change • Marked changes in muscle tone • Choking • Gagging
Definition of ALTE (cont'd) • In some instances, the caregiver has feared that the infant was going to die. • Previous misleading terms such as “near-miss SIDS” or “aborted crib deaths” • Not a diagnosis
Incidence of ALTE • True frequency and prevalence are unknown. • Estimated to be 0.05 to 1% in population-based studies. • Other studies have shown an estimate of up to 6% of all infants or 0.6 to 9.4 in 1000 of live-born infants. • Account for 0.6% to 0.8% of all emergency department visits for children under 1 year of age.
SIDS Peak age 2-4 months Mothers more likely to be under age 20 years Usually occurs between midnight and 6am Decreased incidence with Back to Sleep campaign Low-birth weight and SGA ALTE vs. SIDSNo clear association or link • ALTE • < 2 months of age • No maternal age difference • Usually occurs between 8am and 8pm • No change in incidence with Back to Sleep campaign • ALTE • < 2 months of age • No maternal age difference • Usually occurs between 8am and 8pm • No change in incidence with Back to Sleep campaign Esani et al. Journal of Pediatrics March 2008
Why is an infant with an ALTE episode so worrisome to the medical provider?
Differential Diagnosis • GI • Gastroesophageal reflux • Intussusception, Volvulus, Swallowing incoordination, Incarcerated hernia • Neurologic • Seizures, breath holding spells, Vasovagal syncope, CNS hemorrhage, hydrocephalus, Neuromuscular disorders • ID • RSV/bronchiolitis, Pertussis, UTI, Sepsis, Meningitis, Encephalitis, Pneumonia
Differential Diagnosis (cont’d) • Respiratory • Upper airway obstruction, foreign body aspiration, Immaturity or prematurity, Central hypoventilation syndrome, Vocal cord dysfunction, Laryngotracheomalacia, vascular ring • Cardiac Disease • Arrhythmia (long QT syndrome, WPW), congenital heart disease, cardiomyopathy, myocarditis • Metabolic disorders • IEM, Hypoglycemia, Hypocalcemia, Hypomagnesemia
Differential Diagnosis (cont’d) • Child Abuse • Accidental or intentional poisoning, Non-accidental suffocation, Physical injury, Head injury, Factious illness (MBP) • Other • Developmental delay, Feeding difficulties, Medications, Hypothermia, Anemia, Food Allergy, Anaphylaxis • Normal Behaviors of Infants • Irregular breathing of REM sleep, periodic breathing, respiratory pauses, transient choke, gag, cough during feeding • Idiopathic/Unknown etiology
Most common discharge diagnosis for ALTE: • Idiopathic/Unknown (50% of all ALTE cases) • Gastroesophageal Reflux • Seizure • Lower respiratory tract infection
Evaluation • HISTORY is the most important diagnostic tool • Detailed description of the event including: • position of infant at the time • events leading up to the episode • interventions taken prior to presentation • was infant awake or asleep • Infant's usual behavior with regards to sleep and feeding habits • Pregnancy and Birth History • Developmental History
History (cont'd) • Family history: • siblings with early deaths, rare conditions, or SIDS • Social history: • smokers, substance abuse, medications in the home • Administration of medications prior to event, including OTC meds and homeopathic medications
Evaluation (cont'd) • Physical Examination is the second most important diagnostic tool • Obtain Vital Signs, including Pulse Oximetry • Plot out height, weight, and head circumference • Complete head to toe exam with particular attention to the respiratory, cardiac and neurologic exam • Consider fundoscopic exam
ALTE and GER • Most common diagnosis for an ALTE episode • Direct cause of the respiratory event is likely laryngospasm (resulting response is apnea, bradycardia, swallowing and/or hypertension). • More likely due to reflux when: • Gross emesis occurs at time of ALTE • Episodes occur when infant is awake and supine • The ALTE is characterized by obstructive apnea • Reflux is pathologic when the infant has esophagitis, bleeding, FTT, or pulmonary aspiration. Mousa et al. Testing the association between GER and apnea in infants. Journal of Pediatric Gastroenterology and Nutrition 2005; 41: 169-177
ALTE and SEIZURES • Second most common cause of ALTE • Studies have determined seizures to be etiology of ALTE in up to 15-25% of all diagnosable cases. • Of those that developed chronic epilepsy, 71% returned within 1 month with second ALTE. • Significant predictors of adverse neurologic outcomes are family history of seizures and male gender • Neurological evaluation with first time ALTE is low yield. • Bonkowsky et al. Death, Child Abuse, and Adverse Neurological Outcome of Infants After an Apparent Life-Threatening Event. Pediatrics 2008; 122: 125-131.
ALTE and Infectious Diseases • Third most common cause of ALTE • Pertussis • RSV/Bronchiolitis - • cause for apnea in High Risk Infants: • full term but less than 1 month of age • preterm but less than 48 weeks PCA • infants with h/o apnea prior to evaluation. • any infant with bronchiolitiis may develop apnea as result of respiratory distress, respiratory muscle fatigue or hypoxia. Shah S. Sharieff G, An update on the approach to apparent life-threatening events. Current Opinion in Pediatrics 2007; 19: 288-294.
ALTE and Child Abuse • Few studies done to determine incidence of infants with ALTE that were found to be victims of abuse • Some studies have detected up to 2-3% • Historical clues • Occurs only in presence of single caretaker • Presents with apnea or cyanosis • Infant required CPR • Even though recurrent, a myriad of diagnostic testing is all negative • Siblings may have history of SIDS
The physical exam is normal in up to 85% of infants after an ALTE. NOW WHAT?
Brand et al. Pediatrics 2005 • Looked at yield of diagnostic testing in infants who have had an ALTE • 243 infants who were admitted to large Children's Hospital outside of New York over 32 month period • Of 3776 tests ordered, 669 (18%) were positive but only 224 (6%) contributed to the diagnosis Brand et al. Yield of Diagnostic Testing in Infants Who Have Had an Apparent Life-Threatening Event. Pediatrics 2005; 115: 885-893.
Brain neuroimaging Skeletal survey EEG Echo pneumogram Brand et al. Pediatrics 2005 (cont'd)Useful tests in patients who had a CONTRIBUTORY History and Physical: • CBC, Chemistry Panel, UA and cultures • CSF analysis and culture • Metabolic screening • Screening for respiratory pathogens • Screening for GER • CXR
Brand et al. Pediatrics 2005 (cont'd) • Useful tests in patients who had a NON-CONTRIBUTORY History and Physical: • screening for GER CXR • UA and culture Pneumogram • brain neuroimaging WBC Concluded that broad evaluations for systemic infections,metabolic diseases, and blood chemistry abnormalities are not productive in the group of infants who have a non-contributory history and physical
Diagnostic Studies (cont'd) • Highest diagnostic yield: • Rapid glucose determination • CBC • Urinanalysis and culture • RSV and Pertussis test • EKG • CXR • Consider – dilated fundoscopic exam, brain neuroimaging, urine toxicology screen, lactate, EEG, testing for pathologic reflux
Admission Criteria • Most studies recommend ALL infants with ALTE should be admitted for observation and further evaluation over 24-72 hour period, regardless of the cause of the ALTE and the appearance of the infant at presentation. • Few studies have specifically evaluated admission vs. discharge home criteria
Admission Criteria (cont’d) • No consensus guidelines for admission • Most hospitalizations are done on an individual patient need basis • Further benefits to hospitalization: • Alleviating parental fears and anxiety • CPR training • Possibility of health care provider to witness an episode
Return back to Case Study • 3 week FT female infant presents to the SCVMC ED after experiencing an episode at home where mother found the infant: • Gagging one hour after feeding • Turned limp • Unresponsive for about 45 seconds • Cried spontaneously • In the ED: • Stable vitals • Well appearing • Normal physical exam
What do you tell the ED physician? Case Study (cont'd)
Case Study (cont'd) • Given that the infant has a history significant for ALTE episode consider: • CBC, CRP, Chem 10, UA/U.cx, EKG, CXR • But remember – “Monitoring only” may be appropriate if event was promptly reversible; short-lived, self-limited; baby is stable on initial monitor, and all observed feeds are reassuring • Given infant's age, as well as mother's fear that her baby was going to die, would admit for a minimum of 24 hour period of observation on CR monitor.
Take Home Points Most common etiologies include GER, Seizures, and Lower Respiratory Tract Infection Always consider Child Abuse History is the most important diagnostic tool Most infants should be admitted for period of observation at minimum, but there may be a small subset that can be discharged.