Download
1 / 50
500 likes | 764 Views
TRALI Cases and Chapter Session. Tanya Petraszko MD FRCPC CBS BC & Yukon January 2010. What is Transfusion-related Acute Lung Injury?. Sudden onset of “Acute Lung Injury” occurring within 6 hours of a transfusion Acute Lung Injury Hypoxemia New bilateral chest X-ray infiltrates

E N D
TRALICases and Chapter Session Tanya Petraszko MD FRCPC CBS BC & Yukon January 2010
What is Transfusion-related Acute Lung Injury? • Sudden onset of “Acute Lung Injury” occurring within 6 hours of a transfusion • Acute Lung Injury • Hypoxemia • New bilateral chest X-ray infiltrates • No evidence of volume overload Canadian Consensus Conference Definition. Kleinman et al. Transfusion 2004;44:1774-89
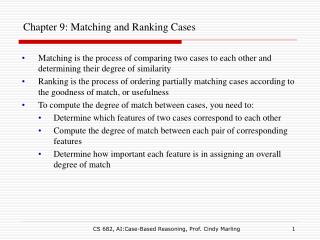
Features of TRALI • SOB and abnormal CXR • Fever, hypotension • onset is usually within the first 1-2 hours of transfusion, but may be delayed up to 6 hours
Normal CXR Patient’s CXR
TRALI Mortality • TRALI appears to be the most common cause of transfusion-related mortality • Reports to the FDA of transfusion-related deaths: • TRALI > bacterial sepsis > acute hemolysis • Estimated rate of fatalities is 5 – 10%
Transfusion Related Fatalities Reported to FDA 2003-2005 Cause#cases (% of fatalities) • TRALI 72 (32%) • Bacterial sepsis 25 (11%) • AHTR 23 (10%) • Other 71 (32%) • Not clearly tx related 34 (15%) • Total 225 (100%)
Leading Cause of Adverse Transfusion Events reported to Health Canada
Evolution of Transfusion Risks HIV and HCV vs TRALI 1 / 102 HIV HCV 1 / 103 Estimated TRALI risk 1 / 104 Transfusion Risk per Unit Estimated TRALI fatality (?) 1 / 105 1 / 106 1984 1988 1992 1996 2000 2004 Adapted from Goodnough L and Aubuchon J
WBC Antibody Hypothesis • Antigen-Antibody reaction triggers TRALI Y Release of substances causing pulmonary endothelial damage and capillary leak Activation Lodged in pulmonary capillaries • Donor • Anti-HNA • Anti-HLA I • Anti-HLA II Recipient WBC - Neutrophils - Lymphocytes - Monocytes Courtesy of Y. Lin
Clinical Correlation • Right, single lung transplant • 10 weeks after transplant, transfused PRBCs for anemia • HLA B44 antibody in PRBC donor • HLA B44 antigen present in lung donor tissue only • Elegant clinical example of targeted endothelial injury from a blood transfusion Dykes et al. Br J Haematol 2000.
What evidence is there for this • Many studies demonstrate HLA or leukoagglutinating alloantibodies in donors • Several examples of donor-recipient antigen/antibody concordance • Anti HLA class I and II implicated • Anti-neutrophil antibodies implicated
Evidence for antibody theory • ex vivo isolated rabbit lung model • severe lung vascular leakage was reproduced using a human anti-neutrophil antibody in the presence of cognate, human 5b-positive neutrophils • In contrast, no vascular leakage was noted in lungs perfused in the absence of either • antibody, • neutrophils, or a • complement source. • No permeability increase occurred with the use of 5b-negative neutrophils • Seeger Blood. 76:1990.
Antibody theory animal models • isolated perfused rat lungs • perfused them with plasma containing anti HNA-2a mAb and human neutrophils. • If neutrophil expression of HNA-2a antigen was >70%, ALI was manifest; • if antigen expression was <30%, ALI was not manifest. • However, if the lungs were primed with fMLP then lung injury was induced in the group with < 30% antigen expression. • Thus, if there is no relevant first hit (priming with fMLP), TRALI may not be manifest even with cognate antibody unless the cognate antigen expression meets a certain threshold. • also demonstrated that anti-HNA 2a directly activates neutrophils in the absence of complement Sachs Blood. 107(3): 2006.
Anti-neutrophil Antibodies (HNA-2a) +FMLP Sachs et al, Blood 2006. Slide from Looney MD, UofC, SF
Non antibody mediated TRALI • 15% of typical TRALI cases fail to demonstrate antibody • alternate hypothesis that some cases may be non-antibody mediated • Biologically active molecules contained in stored blood products • lysophosphatidylcholines • interleukins
What evidence is there for this • Rats pre-treated with LPS developed acute lung injury (ALI) when the lungs were perfused with plasma • Rats did not get ALI with LPS alone • Rats pretreated also got ALI with lipids extracted from stored 42 day old human RBCs or platelets • Did NOT get ALI if given lipids from 5 day product • thus plasma or lipids from fresh, human RBCs or platelets did not cause lung injury. Silliman CC J. Clin.Invest 101(7): 1998 Silliman CC Transfusion. 43: 2003
Two Event Model • Recipients of blood containing anti WBC antibodies don’t all get TRALI • perhaps two events required to manifest TRALI (as in ARDS) • Predisposing clinical condition • Infusion of biologically active mediators
First event results in activation of pulmonary endothelium with neutrophil priming • Second event results in activation of the neutrophils adherent to pulmonary endothelium and subsequent lung injury
Two event hypothesis 2nd event: Transfusion of biologically active lipids or antibodies 1st event: Underlying clinical condition of patient (inflammation, infection, surgery) Activation Release of substances causing pulmonary endothelial damage and capillary leak Activation of pulmonary endothelium with increased adhesion molecules Silliman et al. Blood 2003;101:454-62 Kleinman et al. Transfusion 2004;44:1774-89
Evidence from animal models • 2-event in vivo rat model • first event • saline (NS) or • endotoxin (LPS) • second event • plasma from stored, human packed red blood cells (PRBCs) or • antibodies (OX18 and OX27) against rat MHC Class I antigens • NS treated rats did not develop TRALI • With plasma nor with antibody • LPS treated rats developed ALI • With plasma and with antibody Kelher Blood. 113(9):2009.
Neutrophil depleted rats had experiment repeated and all failed to demonstrate ALI • Confirmed that ALI is neutrophil dependent • also demonstrated that anti-MHC Class I localized to the neutrophil surface • They concluded that TRALI is the result of 2 events with the examples of the second event being plasma from stored blood and antibodies that prime neutrophils.
Case of recurrent TRALI52 year old female 4 months post allo BMT for myelofibrosis; transfusion dependent 2007-02-10 • received 2 units red cells uneventfully as an outpatient. • Discharged but became acutely SOB on way home, returned to ER • CXR showed bilateral new infiltrates • Decreased sats, intubated and ventilated for 30 hours then extubated and recovered. Results of Investigation • Recipient results: post- sample: Negative • Donor 1st unit negative • Donor 2nd unit positive for anti HLA antibody • Crossmatch donor 2 with recipient positive
Case of recurrent TRALI52 year old female 4 months post allo BMT for myelofibrosis; transfusion dependent 2007-03-19 • Had been discharged home receiving regular outpatient transfusions 2x/week • after transfusion of 2 units of RCC developed new onset SOB, new CXR infiltrates and PO2<60. • Required mechanical ventilation. Results of Investigation • Recipient results: pre-samples: positive anti HLA • post-sample: positive anti HLA • No crossmatch done • Donor 1st unit positive anti HLA antibody • Donor 2nd unit positive anti HLA antibody
Two event model • In first TRALI event, implicated donor associated platelet unit did not cause TRALI in the recipient it was given to • That recipient was not primed or did not have cognate antigen….
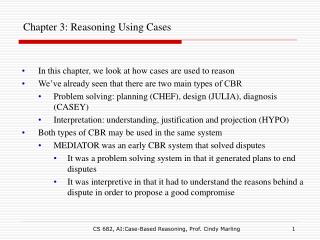
Evidence from animal models • in vivo mouse model • BALB/c wild-type mice positive for MHC Class I antigen were injected with MHC Class I mAb via the jugular vein and sacrificed at 2 hours. • Control mice were knock out mice negative for the antigen • Injection of MHC Class I mAb produced severe ALI in wild type mice with 50% mortality compared to controls negative for the cognate antigen. Looney MRJ. Clin. Invest. 116:(2006)
MHC I antibody produces severe ALI in mice 180 140 BALB/K + MHC I mAb ** ** BALB/c + Isotype control mAb 160 BALB/c + MHC I mAb 120 140 100 120 80 100 EVPE (µl) Excess lung water (µl) 80 60 60 40 40 20 20 0 0 PBS or Isotype control mAb MHC I mAb 100 80 ** 60 Survival (%) 40 20 0 15 30 45 60 75 90 105 120 (Minutes)
Evidence from animal models • The MHC Class I mAb binds throughout the body and prominently in the lung microvasculature. • The investigators demonstrated that this antibody also binds to neutrophils, but does not cause direct neutrophil activation. Looney MRJ. Clin. Invest. 116:(2006)
Evidence from animal models • Mice were also neutrophil depleted with GR-1 antibody • these mice were protected from lung injury. • Thus the absence of circulating neutrophils renders the bound antibody on lung tissue inert and unable to cause vascular permeability. • Using a knockout mouse it was further demonstrated that it was the Fc gamma receptor which was essential in responding to the antibody challenge. • The Fc gamma receptor knock out mice were fully protected from lung injury, however when wild type neutrophils were transfused back, the lung injury was restored. • Thus in this model, • MHC Class I antibody binds to class I antigen on the endothelium • then presents the Fc portion of the antibody to the neutrophil • Neutrophil is then activated thru Fc gamma receptor engagement. • demonstrated a critical role for neutrophil Fc gamma receptors in mediating ALI. Looney MRJ. Clin. Invest. 116:(2006)
Summary so far • Clinical features of TRALI • Leading cause of TR mortality • Majority appear to be antibody mediated • Animal models support this So….why don’t we always see TRALI when antibody and cognate ag are present?
Effect of environment on priming • Mice were housed in specific-pathogen free barrier conditions vs. non-barrier housing • Repeated TRALI model • Barrier mice were protected from TRALI • non barrier mice did develop ALI. • Barrier mice demonstrated lower levels of circulating neutrophils • suggesting that this is the reason why they did not respond to the second hit since this model is neutrophil dependent. • if barrier mice were primed with LPS prior to receiving anti-MHC Class I mAb, then they did develop ALI in a dose-dependent manner. Looney. J Clin Invest. 119(11): 2009
Anti-neutrophil Antibodies (HNA-2a) +FMLP Sachs et al, Blood 2006. Slide from Looney MD, UofC, SF
Role of neutrophils in ALI • microfluidics model of the lung microcirculation. • MHC Class I mAb is immunoadsorbed to the artificial capillary bed, and the unbound antibody is removed by washing. • Next, Fc gamma receptor knockout neutrophils or wild-type neutrophils are perfused. • video demonstrates that Fc gamma receptor knockout neutrophils zip right through the capillaries as they cannot engage the bound antibody • wild-type neutrophils all get stuck as they engage the bound antibody through their Fc gamma receptor.
Effect of hematopoetic cells in priming • hematopoietic chimeras TLR4 mice, which are LPS unresponsive • TLR4 mice reconstituted with TLR4 bone marrow were protected in the two-event model of TRALI (LPS + MHC Class I mAb). • However, when TLR4 mice were reconstituted with wild-type bone marrow, lung injury was manifest • thus demonstrating that hematopoietic cells are the critical population that must be primed to produce lung injury. Looney. J Clin Invest. 119(11): 2009
Conclusions from animal models • Well developed animal models support the two event hypothesis of TRALI. • effective ‘second hits’ in TRALI • Neutrophil or • MHC Class I antibodies or • plasma or lipids from stored, human RBCs • Priming of hematopoietic cells is necessary in experimental TRALI and may be the ‘first hit’. • Common to all experimental models, neutrophils are the key effector cell in TRALI.
How can we prevent TRALI? • We have evidence that antibodies are responsible for TRALI in a primed host • How can we identify a primed host? • Fresher product for the primed host?
How can we prevent TRALI? • TRALI reduction strategies have focused on donors with antibodies and specifically plasma containing products • Secondary – Measures taken to identify the cause of a reaction that has occurred and prevent it from happening again • Primary – Preventive measures taken to eliminate the risk before it happens in the first place
How can we prevent TRALI • Secondary…defer implicated donors • Donors associated with a reported TRALI are investigated for anti HLA and anti neutrophil antibody and deferred if positive • Pilot 2001 – 2006, SOP 2006 • Primary…avoid donors with anti HLA or anti neutrophil antibody • what have blood suppliers done and what has the effect been • Donor loss • Reduction of TRALI
Which donors develop WBC antibodies? • WBC alloimmunization may occur following previous exposure to WBCs through pregnancy or transfusion • 332 female plateletpheresis donors • 17% had detectable anti-HLA antibody • Frequency of HLA antibodies increased with pregnancy: 0 pregnancies: 7.8% 1-2 pregnancies: 14.6% 3 or more: 26.3% Densmore et al. Transfusion 1999;39:103-6
Primary Prevention • 2003 – UK changed component production policy moving to predominantly male plasma for transfusion Chapman et al. Vox Sang 2006;91(Suppl 3):227
SHOT data • 10 years hemovigilance in UK and impact of preferential use of male donor plasma • Risk of highly likely/probable TRALI due to FFP decreased • 15.5 per million units 1999-2004 • 3.2 per million units issued 2005-2006 (p= 0.0079) • Risk of highly likely/probable TRALI due to platelets decreased • 14 per million to 5.8 per million • Chapman.Transfusion 2009;49:440-452
TRALI reduction measures CBS-predominantly male plasma • CBS moved to predominantly male plasma for transfusion Oct 2008 • Female plasma diverted fractionation
TRALI the CBS Experience – Definite and Possible SMH: GIFT, LIFT, LCT, X-Match when possible CBS:Luminex HLA TRALI pilot project CCC January (12hrs) (October) male only plasma TRALI CCC April (6 hours) BC Edmonton (March) BC Toronto (January) BC BC & Y (March)
TRALI Reduction Measures – Platelet Apheresis • On July 20, 2009 CBS started asking all female platelet donors if they’d ever been pregnant • Any responding positively redirected to whole blood
Donor Loss YTD • June 2009 there were 2394 female apheresis platelet donors • By Nov 2009 only 300 active female apheresis platelet donors • 32% of the remaining donors converted to whole blood or plasma (approx 765 donors) • Net loss of approx 1329 donors
F2008/09 reversed the trend of large rises in the number of platelet imports.
TRALI – Platelet Apheresis • In BC, LVPs allowed CBS to continue to meet platelet demand with fewer imports • The number of platelet apheresis units collected since implementation of the TRALI reduction measures has not decreased, in fact increased with 38% growth • BC Yukon data • National growth: 6% • National data: LVP target 34.5% actual YTD 23.4%
Summary Primary Prevention • Reports of TRALI have decreased since shift to male plasma • Consistent with experience elsewhere • Donor loss due to deferral of previously pregnant females largely mitigated by collection of double platelets
Will there be enough snow for the Olympics?? Questions?