Download
1 / 3
30 likes | 132 Views
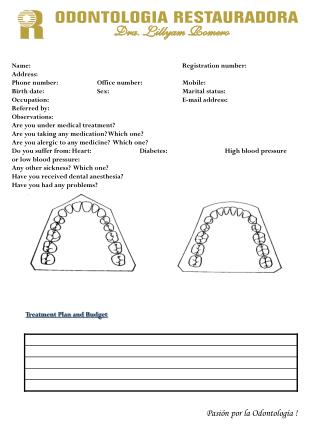
Complete the patient registration form for Dr. Lillyam Romero's dental services, providing essential information and medical history to ensure proper treatment and care. Sign and submit to finalize registration.

E N D
Name: Registration number: Address: Phone number: Office number: Mobile: Birth date: Sex: Marital status: Occupation: E-mail address: Referred by: Observations: Are you under medical treatment? Are you taking any medication? Which one? Are you alergic to any medicine? Which one? Do you suffer from: Heart: Diabetes: High blood pressure or low blood pressure: Any other sickness? Which one? Have you received dental anesthesia? Have you had any problems? Treatment Plan and Budget Pasión por la Odontología !
Before I finish this treatment I have to pay the total cost of it to Dra. Lillyam Romero. Name and signature: ______________________