Download
1 / 35
790 likes | 4.6k Views
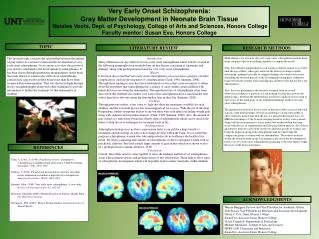
Childhood and Early Onset Schizophrenia. Afshan Anjum, M.D. Assistant Professor Department of Child and Adolescent Psychiatry University of Minnesota. Age of onset during teens and late 20’s, childhood onset is rare. Males have earlier age of onset

E N D
Childhood and Early Onset Schizophrenia Afshan Anjum, M.D. Assistant Professor Department of Child and Adolescent Psychiatry University of Minnesota.
Age of onset during teens and late 20’s, childhood onset is rare. Males have earlier age of onset Both genetic and environmental components involved Diverse array of both cognitive and clinical symptoms Evidence supports a neurodevelopmental hypothesis Drugs of abuse can mimic symptoms of schizophrenia Improvement of positive symptoms with typical neuroleptics Improvement of symptoms and cognition with atypical neuroleptics Schizophrenia – The etiologic puzzle
Schizophrenia in Children and Adolescents • Same criteria as that used for adults • Rare in children • 0.1 to 1% of patients with schizophrenia present prior to 10 years of age. • 4% prior to 15 years of age • Incidence increases after puberty • Peak age of onset between 15 and 30 years of age • 47% display onset (prodromal phase) prior to 21 years of age • 21% have psychotic symptoms prior to age 21.
Genetic Factors Courtesy Dr. Irv Gottesman
Social withdrawal odd or schizotypal preoccupations deteriorating academic performance Worsening hygiene and self-care skills dysphoria Idiosyncratic or bizarre behaviors Increase in aggressive behaviors or other conduct problems Substance abuse Typically the earlier the onset, the more insidious the prodromal phase Prodromal Symptoms of Schizophrenia
Initial and follow-up diagnoses of teenage patients with psychotic symptoms referred to the MH-CRC
Bipolar Affective Disorder Gabrielle Carlson, 2000
Hallucinations Rare under 7 yrs. After 7 yrs. is the most common symptom Auditory ~ 80% Visual 33-46% Delusions Rare under age 7 yrs. 41-86% will have delusions Less complex delusional system in younger children Thought disorder Found in 60-100% of children Illogical thinking and loose associations can be reliably detected Incoherence and and poverty of speech more difficult to assess Blunting of affect in 63% of children Catotonia is rare Child and Adolescent Schizophrenia
Positive Symptoms • Hallucinations • Auditory hallucinations • Voices commenting • Voices conversing • Somatic or tactile hallucinations • Olfactory hallucinations • Visual hallucinations
Positive Symptoms - Delusions Persecutory delusions Delusions of jealousy Delusions of guilt or sin Grandiose delusions Religious delusions Somatic delusions Delusions of reference Delusions of being controlled Delusions of mind reading Thought broadcasting Thought insertion Thought withdrawal
Positive Symptoms • Bizarre behavior • Clothing and appearance • Social and sexual behavior • Aggressive and agitated behavior • Repetitive or stereotyped behavior
Positive formal thought disorder Derailment Tangentiality Incoherence Illogicality Circumstantiality Pressure of speech Distractible speech Clanging Positive Symptoms
Negative Symptoms • Affective flattening or blunting • Unchanging facial expression • Decreased spontaneous movements • Paucity of expressive gestures • Poor eye contact • Affective responsivity • Lack of vocal inflections
Negative Symptoms • Inappropriate affect • Alogia • Poverty of speech • Poverty of content of speech • Blocking • Increased latency of response
Negative Symptoms • Anhedonia - Asociality • Recreational interests and activities • Sexual activity • Ability to feel intimacy and closeness • Relationship with friends and peers
Negative Symptoms • Attention • Social inattentiveness • Inattentiveness during mental status testing • Avolition - Apathy • Grooming and hygiene • Impersistence at work or school • Physical anergia
Verbal memory Nonverbal memory Working memory Language skills visuospatial skills Initiation / Speed Sustained and selective attention Problem solving Motor Neuropsycholgical Domains
Cognitive Function of Adolescents and Adults Compared to Controls
Cognitive Function of Adolescents and Adults Compared to ControlsNeuroleptic Naïve
The Etiology of Schizophrenia:Neurodevelopmental versus Neurodegenerative • A case against neurodegeneration • No evidence of excessive gliosis • A number of studies do not demonstrate progression of the neurobiological findings • Ventricular Brain Ratio • Gray or white matter • Neuropsychological performance
Structural Brain Differences Reported in Previous Studies of Children and Adolescents with Schizophrenia
Medical causes of psychotic symptoms • Metabolic • Renal failure, hepatic failure, pancreatic disease, hyper/hyponatremia, hyper/hypocalcemia, hyper/hypoglycemia, porphyria, dehydration, hyperosmolar states • Endocrinopathies • Addison’s disease, Cushing’s disease, hypo/hyperthyroidism, hyperparathyroidism, panhypopituitarism
Medical causes of psychotic symptoms • Nutritional deficiency states • Thiamine, folate, B12, niacin • Autoimmune disorders • Systemic Lupus Erythematosus, temporal arteritis
Medical causes of psychotic symptoms • Drug Induced • Street drugs(alcohol, hallucinogens, heroin, inhalants, psychostimulants) • Prescription drugs(Steroids, stimulants) • Withdrawal (alcohol, hallucinogens, opiates, psychostimulants, sedative-hypnotics) • Poisoning (Anticholinergics, carbon monoxide, heavy metals)
Neurological causes of psychotic symptoms • Infection • Viral: Herpes simplex, HIV • Syphilis • Parasitic • Neoplasm, CVA, Trauma (especially frontal and temporal) • Degenerative (Alzheimer’s disease, Pick’s) • Seizure (Especially complex partial)
Neurological causes of psychotic symptoms • Motor Disorders • Parkinson’s, Wilson’s, Huntington’s, Sydenham’s chorea, idiopathic basal ganglia calcification, spinocerebellar degeneration • Myelin Disease • Adrenoleukodystrophy, metachromatic leukodystrophy, Marchiafava-Bignami disease, Multiple Sclerosis • Miscellaneous • Hydrocephalus, hypoxic encephalopathy, narcolepsy
History Collateral information is crucial Physical exam Especially neurological examination CNS Studies ? EEG ? Brain imaging Laboratory studies CBC with differential Chemistry profile liver enzymes electrolytes, Mg, Phos, Ca, glucose BUN, Creat. Thyroid function T4, TSH Urinalysis Urine screen for substances of abuse Ruling out medical causes of psychotic and affective syndromes
Schizophrenia Schizoaffective disorder Bipolar Affective Disorder Brief Reactive Psychosis Delusional Disorder Postpartum Psychosis Psychotic Depression Malingering/Factitious Disorder Normal development Substance induced psychosis Borderline Personality Disorder Autism spectrum disorders Communication disorders Obsessive-Compulsive Disorder Schizotypal Personality Disorder Schizoid Personality Disorder Psychiatric Differential Diagnosisof schizophrenia or psychotic symptoms
As the Proton Turns:Normal Brain Development through Adolescence and Early Adulthood • Gray matter pruning • Linear age-related decrease in frontal and parietal regions and subcortical structures (Jernigan et al., 1991) • Cortical GM peaks at age 4 and decreases thereafter (Pffererbaum et al., 1994) • Continued myelination • The association cortex (Yakovlev and Lecours, 1967) and the corpus callosum (Pujol et al., 1993) continues to develop into the third decade of life. • Steady increase in cortical WM volume until the age of 20 (Pffererbaum et al, 1994)
Neuroleptics Mood Stabilizers Anxiolytics PsychoSocial Interventions Psychotherapy Individual Therapy (CBT, CBSST) Family Therapy Psychoeducational Psychotherapy Psychotropic Medications
Prognosis • Stability of Diagnosis • Treatment Response