Download
1 / 100
1.22k likes | 2.18k Views
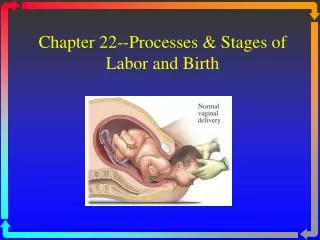
Chapter 12--Processes & Stages of Labor and Birth. Critical Factors In Labor. The Four P’s: passage, passenger, powers & psyche Passage : adequate pelvis? cephalopelvic disproportion (CPD) Suspect if presenting part does not engage in pelvis (0 station). Passenger.

E N D
Critical Factors In Labor • The Four P’s: passage, passenger, powers & psyche • Passage: • adequate pelvis? • cephalopelvic disproportion (CPD) • Suspect if presenting part does not engage in pelvis (0 station)
Passenger • The fetus: head is largest diameter • Fetal head: 4 bones with 3 membranous interspaces (sutures) that allow bones to move & overlap to diminish size of skull • Molding: head becomes narrower, longer, sutures can overlap--normal--resolves 1-2 days after birth • Fontanelles: at junctures of skull bones
Passenger • Fetus and fetal membranes • Molding of head • Fetal lie • Longitudinal • Transverse • Oblique
Fetal Lie and Presentation • Leopold's maneuvers/US • Longitudinal lie: Vertical • Presenting part: • cephalic (head), • vertex (occiput), chin (mentum) • breech (buttocks or feet) (c-section) • sacrum • Transverse lie: Horizontal (c-section) • Presenting part: shoulder (acromion)
Passenger (cont.) • Fetal attitude—flexion • Fetal presentation • Cephalic • Vertex • Military • Brow • Face
Advantages of Cephalic Presentations • Head usually largest part of infant • Molding • Optimal shape—smooth and round
Breech presentation Assessment: FHT heard high on the abdomen, Leopold’s, vaginal exam & US. • Higher risk of anoxia from prolapsed cord, traumatic injury to the after coming head, fracture of spine or arm, dysfunctional labor • Usually delivered by C-section
Disadvantages of Breech Presentation • Risk of cord prolapse • Presenting part less effective in cervical dilation • Risk of cord compression • Risk of prolonged labor
Shoulder Presentation • Occurs when fetus in transverse lie • Cannot be delivered vaginally unless rotation occurs
IMPORTANT TERMS • Effacement: shortening and thinning of cervix • Expressed as a percentage (0% to 100%) • Dilation: opening and enlargement of cervix • Expressed in centimeters (1 to 10 cm)
Station Descent of fetal head (in cm) Effacement Thinning of cervix (in %)
Descent of fetal head: Station Floating Engaged At outlet/crowning
Passageway +Passenger Relationship • Engagement • Station • Ischial spines—0 station • Above ischial spines—(–) minus station • Below ischial spines—(+) plus station • +4 cm means that ...
Powers • Uterine contractions—primary force • Maternal pushing efforts—secondary force • Characteristics of uterine contractions • Increment • Acme • Decrement
Powers Maternal Pushing Efforts • “Bearing down” sensation • Urge to push • No urge to push
Assessment of Uterine Contractions • Characteristics • Frequency • Duration • Intensity • Palpation • Electronic fetal monitoring
Onset of labor • Usually begins between 38 & 42 weeks • Mechanism is unknown • Upper uterus contracts downward pushing presenting part on cervix causing effacement and dilatation • Premonitory signs of labor: • Lightening, Braxton-Hicks contractions (false labor), • cervical changes (ripening), • bloody show (mucous plug), • rupture of membranes (ROM), • sudden burst of energy
False Labor Benign and irregular contractions Felt first abdominally and remain confined to the abdomen and groin Often disappear with ambulation and sleep. Do not increase in duration, frequency or intensity True Labor: Begin irregularly but become regular and predictable Felt first in lower back and sweep around to the abdomen in a wave Continue no matter what the women’s level of activity Increase in duration, frequency, and intensity False vs True Labor:Contractions
False Labor No significant change in dilation or effacement No significant bloody show Fetus- presenting part is not engaged in pelvis True Labor Progressive change in dilation and effacement Bloody show Presenting part engages in pelvis False vs True Labor:Cervix
Critical Thinking • A primigravida client has just arrived in the birthing unit. What steps would be most important for the nurse to perform to gain an understanding of the physical status of the client and her fetus? A. Check for ruptured membranes, and apply a fetal scalp electrode B. Auscultate the fetal heart rate between and during contractions C. Palpate contractions and resting uterine tone D. Perform a vaginal exam for cervical dilation, and perform Leopold's maneuvers E. Determine gestational age of fetus
First Stage of Labor: • 0 to 10 cm: dilatation--opening of cervix) • Latent: slowest part of the process--slow dilation, mild contractions • from onset of regular UCs to rapid dilatation (about 3-4 cms) • Active: labor “picks up steam”--period of more rapid dilation • from 4 cm to full dilatation: stronger UCs • Transition: 7-10 cm--intense, N/V, shaking
Landmarks • Abbreviations are used • First and last letter—maternal pelvis • Middle letter—fetus presenting part • Examples • ROA (right occiput anterior) • ROP • LSP
Psychosocial Influences • Other critical factors • Readiness, educational preparedness, etc. • Cultural views of childbirth • Role transition facilitated by positive childbirth experience • Negative experience interferes with bonding and maternal role attainment
Admission Procedures • Establish positive relationship • Collect admission data • Initial admission assessments • Focused • Psychosocial assessment • Cultural assessment • Laboratory tests
Nursing Care • Ongoing assessment • Facilitate a positive birth experience • Manage discomfort • Advocate for patient’s needs • Provide anticipatory guidance
Initial physical assessment & history Admission--rapport Fetal & UC monitoring Vaginal exams, q 2 hours Vital signs Temperature q 4 hours-intact or q 2 hours ROM Educate regarding labor Encourage comfort, position changes, bladder emptying Assess pain, pain tolerance, preferred type of labor/delivery Reassure regarding what is normal, reduceanxiety • Couple excited, talkative, pain is manageable Care of Laboring Patient Early Labor
Couple quieter, discouraged, pain increasing Care of Laboring PatientActive Labor • Transition (7-10 cm): Yikes! “out of control”, shaking, nausea/vomiting, sweating, pain is intense • Prepare for delivery • Second stage (Pushing): • Educate/instruct regarding pushing • Assess urge to push and fetal descent • Encourage/motivate patient, assess fatigue • Monitor fetal/maternal response to pushing bulge, crowning • Signs of imminent birth: perineal bulging
Labor Support • Presence • Promote comfort • Environment • Personal hygiene • Elimination • Supportive relaxation techniques
Critical Thinking A client is admitted to the labor unit with contractions 2 to 3 minutes apart and lasting 60 to 90 seconds. The client is apprehensive and vomiting. This nurse understands this information to indicate that the client is most likely in what phase of labor? • A) Active • B) Transition • C) Latent • D) Second
Fetal Assessment • Position • Fetal heart sounds • Baseline FHR • Presence of • Variability • Accelerations • Decelerations
Interpretation of FHR Tracings • Consider contraction frequency and intensity, stage of labor, and earlier FHR pattern • Reassuring • Non-reassuring
Nursing Care • FHR decelerations • Early: no action • Variable and late • Lateral position changes • Oxygen per face mask • Palpation for hyperstimulation • Discontinue oxytocin • Increase IVF rate
Second Stage of Labor • Full dilation through birth of infant • Urge to push • Promote effective pushing • Closed-glottis • Open-glottis • Position of comfort
Preparation for Birth • Bulging of the perineum and rectum • Flattening and thinning of the perineum • Increased bloody show • Labia begin to separate
Imminent Birth • Crowning • Burning sensation • Intense pressure in rectum
Mechanisms of labor. A, Descent. B, Flexion. C, Internal rotation. D, Extension. E, External rotation. Cardinal Movements of Birth
Crowning Crowning In the hospital Alternative settings
Nursing Diagnoses for Intrapartal Patient • Pain • Knowledge deficit • Anxiety • Fatigue • Risk for infection • Impaired fetal gas exchange
Third Stage • Birth of baby to complete delivery of placenta • Smaller, spherical uterus • Elevation of uterus in abdomen • Lengthening and protrusion of cord • Gush of blood from vagina
Fourth Stage • Delivery of placenta through 1 to 2 hours after birth • Monitor position and firmness of uterus • “Boggy,” soft uterus • Report immediately • Initiate fundal massage • Assess lochia • Vital signs and urine output • Shivering—offer blankets
Fourth Stage—Risk Signs • Hypotension • Tachycardia • Excessive bleeding • Noncontracting uterus
Chapter 13 Promoting Patient Comfort During Labor and Birth
Pain During Labor and Birth • Shaped by past experiences • Assessing pain • Physiological, psychological indicators • Patient responses • May be intensified by fear, anxiety, fatigue
Physical Causes of Pain Labor and Birth