Download
1 / 44
440 likes | 460 Views
Learn about somatization disorder and its impact on disaster survivors, including diagnostic criteria, comorbidity with trauma, and challenges in studying this disorder post-disaster.

E N D
Disclosure to Participants • Successful Completion of This Continuing Education Event Requires You to: • Complete registration and sign in sheet • Attend entire event • Participate in education activities • Complete participant evaluation • Commercial Support: • This educational activity received no commercial support. • Disclosure of Conflict of Interest: • The speakers and planning committee for this event have disclosed no financial interests. • Non-Endorsement Statement: • Accredited status does not imply endorsement of any commercial products or services by the Department of State Health Services, CE Service; Texas Medical Association; or American Nurse Credentialing Center. • Off-Label Use: • The speakers did not disclose the use of products for a purpose other than what it had been approved for by the Food and Drug Administration. • Expiration Date for Awarding Contact Hours: • Complete the attendance sheet and evaluation by the end of the session. • Other Credits Offered: • Professional Development (PD) for Licensed Psychologists • Continuing Education for Licensed Chemical Dependency Counselors (LCDC) • Social Work/LPC/LMFT • Continuing Legal Education (CLE) • Continuing Professional Education for Accounting (CPE) • CEUs for Certified Peer Specialists (CPS) and Certified Family Partners (CFP)
Disclosure to Participants Continuing Medical Education: The Texas Department of State Health Services, Continuing Education Service is accredited by the Texas Medical Association to provide continuing medical education for physicians. The Texas Department of State Health Services, Continuing Education Service designates this live activity for a maximum of 16.5 AMA PRA Category 1 Credit(s)TM. Physicians should claim only the credit commensurate with the extent of their participation in the activity. This course has been designated by The Texas Department of State Health Services, Continuing Education Service for 3 credit(s) of education in medical ethics and/or professional responsibility. Continuing Nursing Education: The Texas Department of State Health Services, Continuing Education Service is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. The Texas Department of State Health Services, Continuing Education Service has awarded 16.5 contact hour(s) of Continuing Nursing Education.
Somatization disorder and somatoform symptoms in systematically studied survivors of 10 disasters Gus Zhang, MD Assistant professor Department of Psychiatry University of Texas Southwestern Medical Center Carol S. North, MD, MPE, DFAPA Medical Director, The Altshuler Center for Education & Research, Metrocare Services The Nancy and Ray L. Hunt Chair in Crisis Psychiatry andProfessor of Psychiatry University of Texas Southwestern Medical Center
Somatization disorder Well-validated diagnosis Multiple medically unexplained somatoform symptoms throughout multiple organ systems Mostly occurs in women 1% prevalence in general population Onset usually before age 30 High levels of medical utilization, hospitalizations, diagnostic tests, procedures, doctor shopping Chronic, lifelong illness Removed in DSM-5 (but remains in population) Somatic symptom disorder (SSD) in DSM-5 describes a different construct
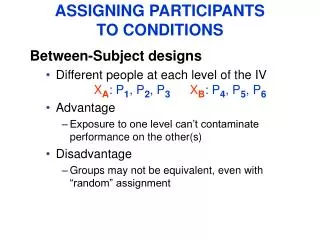
Somatization disorder and trauma Patients with somatization disorder often have extensive trauma history Somatization disorder often comorbid with other psychiatric disorders, including mood disorders, anxiety disorders and post-traumatic stress disorder (PTSD) Studies examining associations between somatization disorder and trauma often suffer from bias - Somatization disorder and other preexisting psychiatric disorders may increase vulnerability to exposure to traumatic events Studying trauma specific to disaster exposure can reduce confounding
Importance of studying disasters Disasters are more likely random and equal-opportunity events, reducing confounding Disasters occur frequently. FEMA shows 50-100 declared disasters per year in US, > 1 per week Local/regional disasters without federal declaration are even more common Disasters can affect any community Disasters have adverse mental health consequences on affected populations Studying psychopathology after disaster is important to inform disaster response and implementation of mental health interventions
Challenges of studying disasters Disasters are challenging to study: Unexpected events, little time to prepare studies Chaotic aftermath, logistical difficulties, identification of survivors Lack of funding Therefore, many disaster studies: Have low sample size Have sample without direct exposure Lack prospective predisaster data Lack unexposed comparison group Use symptom checklists instead of structured diagnostic instruments
Methods 811 directly exposed survivors of 10 disasters in the United States Largest study of somatization disorder in aftermath of disaster to date 3 types of disasters represented: natural disasters (flood, tornado, earthquake), accidents (firestorm, plane crash), and crime/terrorism (mass shootings, bombing) Used same research protocol and assessment methods at each site, allowing databases to be combined Interviews conducted in early postdisaster period, at a median of 3 months after disaster Diagnostic interview schedule (DIS) administered at all sites to assess for MDD, PTSD, panic disorder, generalized anxiety disorder, alcohol use disorder, and somatization disorder (data on diagnoses other than somatization disorder published in other articles, but included here)
Methods - cont Disaster supplement to DIS (DIS/DS) administered at all sites to assess for variables related to exposure Assessment of somatization disorder included 35 individual somatization symptoms Probe flowchart algorithm allowed for characterization of these symptoms (medically unexplained or not) Onset and recency variables allowed for determination of predisaster and postdisaster prevalence and incidence for psychiatric disorders as well as individual symptoms Data analyzed with SAS 9.3 α=.05
Results – somatoform symptoms Mean lifetime number of symptoms per person by symptom category
Results – somatoform symptoms Frequency table of number of somatoform symptoms (predisaster, postdisaster, and incident) with corresponding percentages of the sample aMaximum=12 bMaximum=7 cMaximum=6
Results – somatoform symptoms Pre and postdisaster prevalence and postdisaster incidence of individual somatoform symptoms
Results – bivariate assocations Incidence of any somatoform symptoms was significantly associated with: Female sex (p < .001) Age < 65 (p = .007) Incidence of MDD (p < .001) Incidence of PTSD (p < .001) Incidence of panic disorder (p < .001) Incidence of GAD (p = .007)
Results – multivariate associations In a multiple logistic regression model with several independent covariates entered simultaneously (age, sex, preexisting psychopathology, disaster related PTSD, and postdisaster MDD), incidence of any somatoform symptoms was predicted by female sex, disaster-related PTSD, and postdisaster MDD independent of other variables.
Discussion Most somatic symptoms have medical explanations, are not somatoform Postdisaster incidence of somatoform symptoms is uncommon Incidence of symptoms was predicted by sex, postdisaster MDD and disaster-related PTSD Even in those with incident symptoms, the mean number of symptoms is low Somatization disorder itself is not an observed outcome of disaster Symptom checklists cannot substitute for structured diagnostic interviews
Problems with symptom checklists Most existing studies of somatization in disaster use one of the following symptom checklists: Clinical Assessment in Neuropsychiatry (SCAN), Brief Symptom Rating Scale (BSRS), Symptom Checklist-90, either the original (SCL-90) or the revised (SCL-90-R) version, Brief Symptom Inventory (BSI), General Health Questionnaire (GHQ) and the Stockholm Somatic Symptom Checklist (SSSC). SCAN and BSRS do not assess for full DSM diagnostic criteria SCL-90, BSI, GHQ, and SSSC do not assess timing of symptom onset or remission needed to identify incident symptoms SCL-90, BSI, GHQ, and SSSC do not distinguish between medically explained vs unexplained symptoms
Discussion Existing literature on somatization disorder after disaster lacks consensus Only 3 other studies used structured diagnostic interviews; 12 studies used symptom checklists Studies using symptom checklists report varying results, difficult to interpret 10 of 12 studies using symptom checklists describe some degree of somatization associated with disaster All 3 studies using structured diagnostic instruments did not find more somatization disorder Our results are consistent with studies using structured diagnostic interviews
Discussion Although somatization disorder is not observed postdisaster, disasters do have adverse mental health consequences PTSD has highest postdisaster prevalence and incidence MDD has second highest postdisaster prevalence and incidence Alcohol use disorder has moderate postdisaster prevalence, but very little incidence. Most alcohol use disorder is pre-existing Postdisaster prevalence and incidence of other psychiatric disorders is very low These findings have been very consistent across disasters studied with similar methods People are resilient. 1 in 3 have any postdisaster disorder, but only 1 in 5 have incident postdisaster disorders
Acknowledgement This study was supported by grant MH40025 from the National Institute of Mental Health and a grant from the National Hazards Research and Applications Information Center, Boulder, CO.
References 1. North CS, Yutzy SH, Goodwin DW. Somatization disorder (hysteria). In: Goodwin and Guze's Psychiatric Diagnosis, 6th ed. New York, NY: Oxford University Press; 2010:207-226. 2. Feighner JP, Robins E, Guze SB, et al. Diagnostic criteria for use in psychiatric research. Arch Gen Psychiatry. 1972;26:57-63. 3. North CS. Somatization in survivors of catastrophic trauma: a methodological review. Environ Health Perspect. 2002;110(suppl 4):637-640. 4. Lenze EJ, Miller AR, Munir ZB, et al. Psychiatric symptoms endorsed by somatization disorder patients in a psychiatric clinic. Ann Clin Psychiatry. 1999;11:73-79. 5. North CS, Kawasaki A, Spitznagel EL, et al. The course of PTSD, major depression, substance abuse, and somatization after a natural disaster. J Nerv Ment Dis. 2004;192:823-829. 6. Escobar JI, Canino G, Rubio-Stipec M, et al. Somatic symptoms after a natural disaster: a prospective study. Am J Psychiatry. 1992;149:965-967. 7. Wahlstrom L, Michelsen H, Schulman A, et al. Longitudinal course of physical and psychological symptoms after a natural disaster. Eur J Psychotraumatol. 2013;4. doi: 10.3402/ejpt.v4i0.21892. 8. Desai NG, Gupta DK, Srivastava RK. Prevalence, pattern and predictors of mental health morbidity following an intermediate disaster in an urban slum in Delhi: a modified cohort study. Indian J Psychiatry. 2004;46:39-51. 9. De Soir E, Versporten A, Zech E, et al. Does exposure type impact differentially over time on the development of mental health disturbances after a technological disaster? Arch Public Health. 2015;73:20. 10. Bromet EJ, Havenaar JM, Gluzman SF, et al. Psychological aftermath of the Lviv air show disaster: a prospective controlled study. Acta Psychiatr Scand. 2005;112:194-200. 11. Bland SH, Valoroso L, Stranges S, et al. Long-term follow-up of psychological distress following earthquake experiences among working Italian males: a cross-sectional analysis. J Nerv Ment Dis. 2005;193:420-423. 12. Wang X, Gao L, Zhang H, et al. Post-earthquake quality of life and psychological well-being: longitudinal evaluation in a rural community sample in northern China. Psychiatry Clin Neurosci. 2000;54:427-433.
References 13. Karanci AN, Rüstemli A. Psychological consequences of the 1992 Erzincan (Turkey) earthquake. Disasters. 1995;19:8-18. 14. Liao SC, Lee MB, Lee YJ, et al. Association of psychological distress with psychological factors in rescue workers within two months after a major earthquake. J Formos Med Assoc. 2002;101:169-176. 15. Papanikolaou V, Adamis D, Mellon RC, et al. Psychological distress following wildfires disaster in a rural part of Greece: a case-control population-based study. Int J Emerg Ment Health. 2011;13:11-26. 16. Sezgin U, Punamäki RL. Earthquake trauma and causal explanation associating with PTSD and other psychiatric disorders among South East Anatolian women. J Affect Disord. 2012;141:432-440. 17. Bromet EJ, Goldgaber D, Carlson G, et al. Children's well-being 11 years after the Chornobyl catastrophe. Arch Gen Psychiatry. 2000;57:563-571. 18. Chung MC, Easthope Y, Eaton B, et al. Describing traumatic responses and distress of community residents directly and indirectly exposed to an aircraft crash. Psychiatry. 1999;62:125-137. 19. Robins LN, Fischbach RL, Smith EM, et al. Impact of disaster on previously assessed mental health. In: Shore JH, ed. Disaster stress studies: new methods and findings. Washington, DC: American Psychiatric Press; 1986:21-48. 20. Smith EM, Robins LN, Przybeck TR, et al. Psychosocial consequences of a disaster. In: Shore JH, ed. Disaster stress studies: new methods and findings. Washington, DC: American Psychiatric Press; 1986:50-76. 21. North CS, Oliver J, Pandya A. Examining a comprehensive model of disaster-related posttraumatic stress disorder in systematically studied survivors of 10 disasters. Am J Public Health. 2012;102:e40-e48. 22. North CS, Ringwalt CL, Downs D, et al. Postdisaster course of alcohol use disorders in systematically studied survivors of 10 disasters. Arch Gen Psychiatry. 2011;68:173-180. 23. Robins LN, Helzer JE, Cottler L, et al. The NIMH Diagnostic Interview Schedule, Version III, Revised. St. Louis, MO: Washington University; 1989.
References 24. Robins LN, Cottler LB, Compton WM, et al. Diagnostic Interview Schedule for DSM-IV (DIS-IV), Version 4.2. St. Louis, MO: Washington University; 1998. 25. Robins LN, Helzer JE, Croughan J, et al. National Institute of Mental Health diagnostic interview schedule. Its history, characteristics, and validity. Arch Gen Psychiatry. 1981;38:381-389. 26. Wing JK, Babor T, Brugha T, et al. SCAN. Schedules for clinical assessment in neuropsychiatry. Arch Gen Psychiatry. 1990;47:589-593. 27. Lee MB, Lee YJ, Yen LL, et al. Reliability and validity of using a brief psychiatric symptom rating scale in clinical practice. J Formos Med Assoc. 1990;89:1081-1087. 28. Derogatis LR, Lipman RS, Covi L. SCL-90: an outpatient psychiatric rating scale—preliminary report. Psychopharmacol Bull. 1973;9:13-28. 29. Derogatis LR, Melisaratos N. The brief symptom inventory: an introductory report. Psycho Med. 1983;13:595-605. 30. Goldberg DP, Hillier VF. A scaled version of the General Health Questionnaire. Psycho Med. 1979;9:139-145. 31. Keskinen-Rosenqvist R, Michélsen H, Schulman A, et al. Physical symptoms 14 months after a natural disaster in individuals with or without injury are associated with different types of exposure. J Psychosom Res. 2011;71:180-187.