Peripheral Arterial Disease SVS Clinical Research Priorities
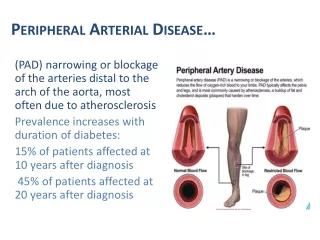
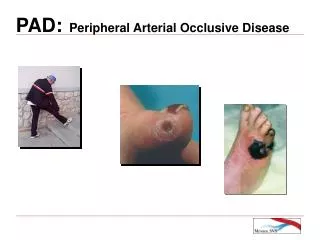
Peripheral Arterial Disease (PAD) affects 8-12 million Americans, especially those over 65 years, with significant societal impacts due to high costs and poor clinical outcomes. This research highlights the need for improved understanding of PAD epidemiology, clinical technology, and patient-centric outcomes, revealing high costs associated with PAD management in the U.S. It also discusses the role of emerging technologies and the importance of exercise and best medical therapy in treating PAD. Future research should prioritize cohesive reporting standards and the exploration of diverse revascularization strategies.

Peripheral Arterial Disease SVS Clinical Research Priorities
E N D
Presentation Transcript
Peripheral Arterial DiseaseSVS Clinical Research Priorities Michael C. Stoner, MD East Carolina Heart Institute East Carolina University Department of Cardiovascular Sciences Brody School of Medicine
PAD Epidemiology • 8 – 12 million Americans • 12 – 15% of population over 65 years Allison JVS 2009. Ciriqui Circulation 2005. Selvin Circulation 2004. Hirsch Vasc Med 208.
HI LI Limb Salvage (CLI pts) P < 0.05 Durham JVS 2010.
PAD Clinical Impact • REACH registry – poor outcomes with concomitant cor and PAD • Many asymptomatic PAD cases, marker of atheroscleortic disease burden • Poorly understood societal impact • Claudication – <1% limb loss rate / year • CLI – 25% Mahoney Circ CV Qual Outcomes 2010.
Cost of PAD • $7 – 8 billion – Medicare expenditure • $151 billion – Total US healthcare system • $14.3 billion – Inpatient CLI care • $10.2 billion – Inpatient PAD care Hirsch Vasc Med 208.
PAD Technology • Rapid expansion of under-studied devices • High-quality trials expensive and may lack external validity • Lateral diffusion of technology across specialties • Provider and institution-bsaed supply-driven model • Lower extremity stent implants • 386,000 529,000 over last 5 years
Cost-efficacy • Impact of initial revascularization strategy? • Driven by durability and longitudinal cost-of-care • Initial procedural cost and resource utilization likely favors endovascular-first • Long-term implications unknown
Open Endovascular TASC II C+D SFA $12,366 ± 496 $7,540 ± 416 $335 ± 150 $226 ± 85 Stoner JVS 2008.
Comprehensive review • SVS CE committee / Mayo systematic review • 1,371 candidate studies 19 papers Moriarty JVS 2011 in press.
Non-standardized • No coherent set of reporting or outcome variables • May favor bypass-first over time • Reporting standards? Moriarty JVS 2011 in press.
CLI strategy Critical Limb Ischemia Bypass Endovascular OPTIMIZE Healing Amputation
BASIL 2005 Adam Lancet 2005.
BASIL 2010 Trend BSX advantage after 24 months Bradbury HTA 2010.
BASIL • High-quality RCT, however… • May lack external validity (technological advancement) • Trend towards BSX better outcomes • Lacking patient-centric outcome • Early cost advantage of ET lost over time (re-intervention) • Role for survival prediction models
CLI strategy Critical Limb Ischemia PRIMARY AMPUTATION? Bypass Endovascular Healing Amputation
Primary amp • Stroke / debilitated patient • Atretic limb • Flexion contracture • Functional dependence • What factors predict failure from CLI revascularization attempt? • Should these patients be counseled for amputation? Commonly cited in (sparse) literature SottiuraiSemVascSurg 2007.
Surgeon v. Patient endpoints 75% Patency 89.5% Limb salvage 96% Survival Traditional 52.6% fully functional 31.6% partially functional 13.2% totally dependent Patient-centric Kumar Ann VascSurg 2011.
Functional status and success • a priori functional status key • Patient-centric when is amp better? Some portion of this 59.1% are better off with amp Taylor JVS 2009. Taylor JVS 2006.
Functional status and BKA Agle SCVS 2009.
Rehab – composite failure Agle SCVS 2009.
Role of emerging technologies Goodney JVS 2009.
Endo tech data void • Explosion of new catheter-based devices • Industry-sponsored and single-center trials • Lesion-based endpoints • May not scale to re-world practice • Often with historical controls • Restricted study populations • i.e. LACI trial and ESRD
Atherectomy in the real-world LACI – 92% 52% • Less dissection & stent use • PTA w/ selective stent = ATH • ? Cost differential Semaan VES 2010. Stoner JVS 2007.
Best medical therapy • Anti-platelet, statin, ACEI/ARB, cilostazol, smoking cessation – all have role • ~40m over 2y • No baseline correlates of success PandeVasc Med 2010.
Exercise & PAD Our patients McDermott JAMA 2009.
Exercise v. Endovascular Spronk Radiology 2009.
Exercise PTA • Optimized patient population • QoL (SF36) measures NS Greenhalgh EJVES 2008.
CLEVER trial • Aortoiliac disease • Moderate-severe claudicants • Best medical therapy (20%) • PTA / Stent (40%) • Exercise (40%) Murphy JVS 2009.
CLEVER outcomes • Primary Endpoint— MWD on graded treadmill test (Gardner protocol) • Secondary Endpoints— Community-based walking (pedometers), QoL, cost-effectiveness, cardiovascular disease risk markers (BMI, waist circumference, lipid profile, blood pressure, glycemic control) Murphy JVS 2009.
Endovascular surveillance • Mismatch between symptoms and duplex velocity? • Criteria for re-intervention unclear Bui JVS 2011.
PAD & data shortcomings • Outcome measures patient centric • Claudication: QoL and walking measures • CLI: MALE, functional status, ambulatory status, longitudinal resource use • Poor adherence to clinical reporting standards • Patient or modality-based?
PAD and new devices • Device-specific versus Patient-specific outcomes • TLR? Binary restenosis? LLI? • Especially with cell-based therapies • Cost and utilization of new technology • Current literature dated, and sparse • Longitudinal databases; ? Role for VQI • Development of reference data for FDA
Treatment effectiveness • Episodic or global payment models • PAD treatment is chronic disease management • Patient, anatomic and socioeconomic correlates of success/failure • Define role of medical optimization at all stages • The workup “imaging cascade”
![Diffuse Vascular Disease (Focus on Peripheral Arterial Disease [PAD])](https://cdn1.slideserve.com/3363465/slide1-dt.jpg)