Download

1 / 32
320 likes | 457 Views
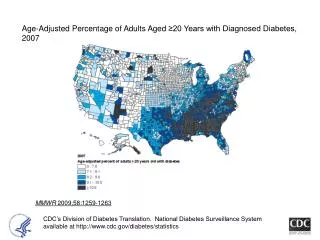
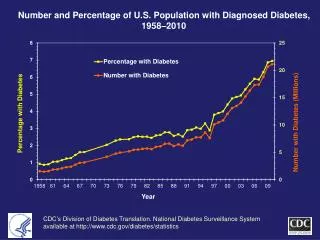
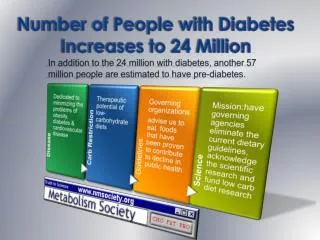
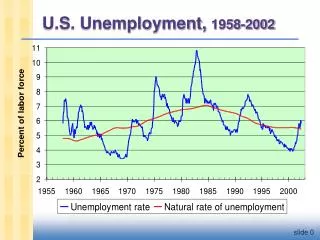
Number and Percentage of U.S. Population with Diagnosed Diabetes, 1958-2008. CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics. 23.6 Million Americans have Diabetes (8% pop) More have pre-diabetes.

E N D
Number and Percentage of U.S. Population with Diagnosed Diabetes, 1958-2008 CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available athttp://www.cdc.gov/diabetes/statistics
23.6 Million Americans have Diabetes (8% pop) More have pre-diabetes
Inherited Forms of Diabetes Mellitus MODY GENES like Mutant glucokinase insulin gene TFs K+channel of the b cell. IR some mitochondria genes
Of 20+ million Americans with Diabetes, only 10% have typeI diabetes
Most diabetics Have Type II diabetes
Type II diabetes Defined by insulin resistance insulin resistance-inability to respond to insulin
Medications for T2DM Many types of diabetes pills can help people with T2DM lower their blood glucose. Each type of pill helps lower blood glucose in a different way. Sulfonylureas- stimulate your pancreas to make more insulin.Biguanides decrease the amount of glucose made by your liver. METFORMINa glucosidase inhibitors slow the absorption of the starches you eat.
Medications for NIDDM Thiazolidinediones TZDs-make you more sensitive to insulin. Meglitinides -stimulate your pancreas to make more insulin.D-phenylalanine derivatives -help your pancreas make more insulin quickly.Combination oral medicines put together different kinds of pills.
Gila monsters are one of only two venomous lizards in the world, the other being the closely related beaded lizards
A fairly new diabetes treatment from Eli Lilly and Amylin that is extracted from the saliva of the Gila monster received approval from the Food and Drug Administration in April 2005 Byetta, which was co-developed by both companies, improves blood sugar control in patients with type 2 diabetes. The drug, developed from a compound in the toxic saliva of a rare lizard found only in the Southwest U.S. and Mexico. Came on Market in June of 2005 Used in patients who aren't getting enough insulin through oral medication
DRAWBACK: Has to be injected (at first was twice a day)
Some History • 1980s an endocrinologist named Dr. John Eng worked of the VA Medical Center in the Bronx His mentor - Dr. Rosalyn S. Yalow, won the 1977 Nobel Prize in Physiology or Medicine for the development of RIAs of peptide hormones. • Dr. Eng wanted to discover new hormones. RIA are insensitive and not a good way to discover new hormones. But chemical assays are sensitive. So he developed a new type of chemical assay and looked for hormones that no one had discovered.
Some History • Dr. Eng first discovered a new hormone in the venom of the Mexican beaded lizard, which in 1990 he named exendin-3. But this hormone was vasoactive, which means that it contracts or dilates blood vessels. • Prompted Dr. Eng to look at the venom of the Gila monster, which is not vasoactive. There he discovered a hormone, which he named exendin-4, that was similar in structure to glucagon-like peptide 1 (GLP-1).
Some History • GLP-1 regulates blood glucose and satiety, as a potential drug it has a short half-life requiring multiple daily injections. He published his key paper on exendin-4 in a 1992 issue of The Journal of Biological Chemistry. • But exendin-4 works for 12 or more hours. "That's how it is better," Dr. Eng says. So, Amylin Pharmaceuticals invested millions of dollars to develop it.
Some History • When Dr. Eng began to realize exendin-4's potential to control diabetes, he told the Department of Veterans Affairs that the agency should patent it. " VA declined, because at that time inventions must be veteran specific," he recalls. The VA did retain a royalty-free license. • "That put me in a difficult position," he says, "because it meant I had to essentially make a bet. Patenting it came out of my pocket with no guarantee that anything would come of it. I ended up with this patent, and I couldn't develop it. So I went around to drug companies."
Some History • Finally, in 1996, Dr. Eng licensed the patent to Amylin, which calls it AC2993. The company completed the Phase 1 study in 1998 and filed an investigational new drug application with the FDA in 1999. Phase 2 studies, announced at the ADA's 2001 Annual Meeting, showed an approximate 1% reduction in A1c after 28 days. Since A1c measures average blood glucose of the past 2-3 months, this is a lot. • Amylin had success in Phase 3 trials.
Some History • Used by 2 injections a day. "The initial target population is for people with T2DM who have not progressed to taking insulin," "It stimulates insulin production when it is needed and is only active when glucose is high." It also reduces appetite, causing some weight loss. • Amylin is also working on alternatives to shots and a long-acting formulation of one shot a month, AC2993 LAR.
Some History • Who would have imagined that a Gila monster could be so valuable to people with diabetes? But Dr. Eng did. Ironically, the venom he worked with came from a lab in Utah, and he says he has never seen a Gila monster.
Not as many proteins as we thought. Not surprising we have some "super-genes“like one that encodes glucagon (increases glucose). As it turns out, the gene for glucagon also codes for at least 2 other hormones, called glucagon-like peptides 1 and 2 (GLP-1, GLP-2). Not only do the GLPs come from the same gene as glucagon, but have a very similar aa sequence as well. Despite these parallels, the GLPs have very different functions than glucagon, and there is a lot of excitement about using these hormones to treat problems ranging from diabetes and obesity to chemotherapy-induced intestinal damage.
From a diabetes perspective, the interesting GLP is GLP-1. GLP-1 is secreted from cells in the gut in response to a meal, and helps to integrate many of the normal physiological responses that occur after eating. For one, GLP-1 induces insulin secretion from the pancreas, and simultaneously reduces glucagon release. This release of insulin actually seems to occur only when the ambient glucose concentration is high, thus reducing the chance that hypoglycemia will develop (an especially attractive feature in a diabetes therapy).
Over a longer period, GLP-1 actually increases the number of insulin-producing b cells. GLP-1 also acts directly on the GI tract, reducing the rate at which food spills out of the stomach and into the SI, making the absorption and storage of energy more efficient.
Finally, and perhaps most intriguingly, GLP-1 acts on the CNS to signal a sense of fullness so that we don't overeat.
Why isn’t GLP-1 prescribed to everyone with T2DM? Well, there are a few problems, The most daunting has been that our bodies destroy GLP-1 within a few minutes. Has to be given orally The enzyme that destroys GLP-1 is called dipeptidyl-peptidase IV (DPP IV), and intense focus has been placed on figuring out ways to disable the enzyme so that GLP-1 can do it's thing for longer periods of time.
One way to get around the problem of DPP IV is to administer a form of GLP-1 that is resistant to destruction. Such forms of GLP-1 have already been found, and the source is he poisonous saliva of the Gila monster lizard. GLP-1 (called exendin-4) from these reptiles has a few key differences from the form found in humans, one consequence of which is immunity to DPP IV. pharmaceutical companies made synthetic forms of exendin-4 (one imagines that it's easier to make the chemical from scratch than it is to harvest toxic lizard spit). Phase 2 clinical trials of exendin-4 in patients with T2DM showed improvements in hemoglobin A1c levels comparable to those seen with currently available ant diabetic drugs. Other studies show reductions of caloric intake after exendin-4 administration.
Another strategy that was pursued is the use of drugs that will inhibit DPP IV directly. Januvia, the first DDPIV inhibitor on the market Studies have shown that 24 hours after taking such a drug, patients with mild T2DM have reduced fasting, post-meal, and average blood sugar levels. The primary advantage of this approach (vs. exendin-4) is that DPP IV inhibitors can be given orally. On the other hand, DPP IV affects other hormones besides GLP-1, and there is concern that blocking the enzyme could cause other problems. One reassuring piece of data is that mice that are genetically engineered to lack DPP IV are viable and appear to do well, and this provides some reassurance that the strategy is sound. Still, longer term studies with both DPP IV inhibitors need to be performed to assess possible toxicity. It is also unclear if the beneficial effects of GLP-1 will be sustained over time, and this too will have to be tested. Nonetheless, a drug that that causes weight loss as well as improved insulin secretion in type 2 diabetes is a potential blockbuster.
April 2010 UPDATE There are 23 DDPIV inhibitors in various stages of development. In monotherapy comparisons with metformin, the DPPIV inhibitors have equal reduction in HgA1c at one and two years. Since neither has dramatic reduction in HgA1c, they will probably be used in combination with other oral agents such as metformin, e.g. Januvamet. Very importantly, they will likely be used for patients with impaired glucose tolerance and for the elderly.
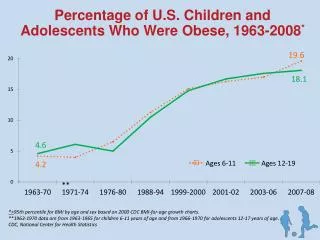
Most patients with Type II diabetes are obese > 85%
Adipocytes accumulate lipid accumulate lipid insulin sensitive insulin sensitive Endocrine functions Endocrine function