Follicular Tracking
how to monitor follicle in ART, IVF

Follicular Tracking
E N D
Presentation Transcript
Follicular Tracking Dr. Samina Khalid SIRM
Introduction • Follicular tracking (a.k.a. follicular monitoring) is the serial ultrasound assessment of ovarian follicles during the follicular phase of a menstrual cycle to monitor their growth and predict ovulation timing. • The follicular maturity can be assessed by estradiol levels which was used previously but frequent measuring can be inconvenient. • Nowadays 3D ultrasound is done which helps in better assessment of the follicles vascularity and maturity • Color Doppler is emerging as an important diagnostic modality during IUI and IVF to assess the uterine , endometrial, and follicular blood flow which are useful markers in predicting the uterine receptiveness, follicular maturity and pregnancy outcome. • Pulsatility index (PI) and resistive index (RI) are popular indexes to assess the flow characteristics of vascular system in ultrasound.
Good pre-HCG Follicle on Color Doppler • On pulse Doppler , these blood vessels show an RI of 0.4 to 0.484 and PSV of >10cm/sec • When functionally mature on color Doppler, the follicle shows blood vessels covering at least 3/4th of the follicular circumference.
Significance of follicular monitoring • To find optimal time for ovulation and reduce guesswork. • To adjust dosage of drug as some patients are hyper responders while others are poor responders. • To avoid excess stimulation leading to OHSS and multiple pregnancy. This helps in: ✔ Increases chances of conception✔ Reduces guesswork in timing✔ Improves outcomes in ART cycles https://www.wombsfertility.com/services/ovulation-induction-follicular-monitoring/?utm_source=chatgpt.com
Physiology behind follicular tracking • Follicle development phases: • Early follicular phase: multiple small follicles begin to grow • Dominant follicle emerges: only one (or few) continues to maturity • Ovulation: mature follicle (~18–24 mm) releases egg ~24–48 hrs after LH surge • Growth rate: ~1–3 mm per day in late development
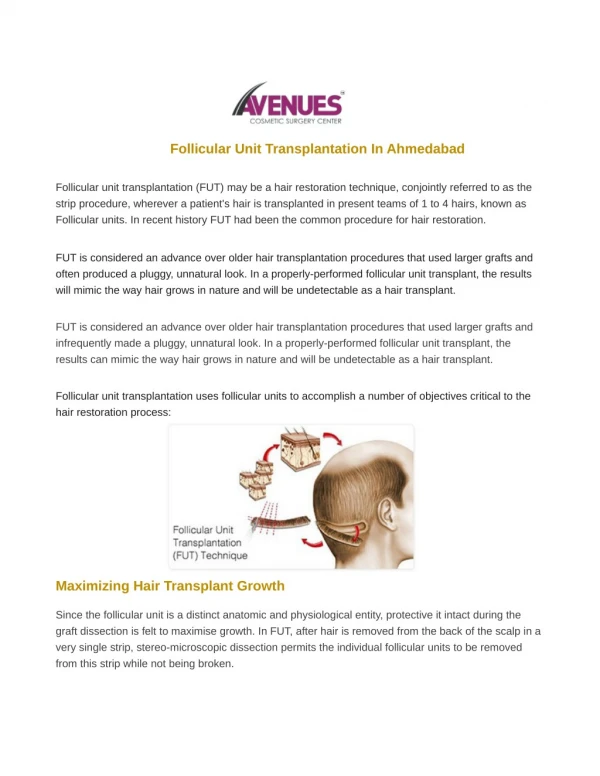
Techniques • Transvaginal ultrasound (TVUS) is the preferred technique: • High-resolution imaging of ovaries and follicles • Serial measurements track growth over time • Endometrial thickness is also monitored • Typical schedule: • Start in early follicular phase (cycle day ~3–10) • Follow-up every 1–3 days as ovulation nears • Daily scans may be needed at peak growth.
Factors for successful Treatment • Ovulation: follicle collapsed, irregular margin, fluid in POD Antral follicle number: Normal AFC is 5-12 follicles per ovary, measuring 2-10mm • AFC <3 high chance of failure Timing: day 2-4 Or 2-5 day of menstrual cycle. • Ovarian stromal blood flow: good predictor of ART success
OHSS • Complication of ovarian stimulation • Consists of: weiht gain, ascites, pleural effusion, oligouria, hemoceoncentration
Predicitng OHSS • More than 4 follicles >16mm Or More than 8 follicle >12mm Risk Factors • Polycystic ovary syndrome (PCOS) • Young age (<35 years) • High antral follicle count (AFC >20) • Large number of developing follicles (>15–20) • Elevated serum estradiol (>3000 pg/mL) • Use of hCG for ovulation trigger or luteal support
Diagnostic criteriaClassification based on RCOG and ESHRE severity criteria.
Management of OHSS • Mild OHSS • Outpatient management • Adequate oral hydration • Analgesia and activity modification • Close follow-up • Moderate OHSS • Frequent clinical and ultrasound monitoring • Fluid balance assessment • Consider hospital admission if symptoms worsen
Severe / Critical OHSS • Hospitalization mandatory • Intravenous fluids (guided by hematocrit and urine output) • Thromboprophylaxis with low-molecular-weight heparin • Paracentesis for symptomatic ascites • Monitor renal, hepatic, and respiratory function • Intensive care support if required
Preventing OHSS • Individualized ovarian stimulation protocols • Use of GnRH agonist trigger instead of hCG in high-risk patients • Cycle cancellation or “freeze-all” embryo strategy • Avoid hCG luteal support in high-risk cycles
Latest guidelines • 1) National Clinical Practice Guidelines (IUI Monitoring) • Ultrasound monitoring recommendations:• All IUI cycles should be monitored with transvaginal ultrasound scans to assess follicular response. • Timing of scans:• In stimulated IUI cycles (with clomiphene/letrozole): Perform baseline scan on cycle day 2–3 to rule out cysts, then serial scans from day 8–10 until trigger day. • Triggering & follicle size thresholds:• hCG trigger is given when at least one dominant follicle reaches: • 20–22 mm in clomiphene/letrozole cycles • ≥18 mm in gonadotropin-stimulated cycles
IUI timing after trigger:• IUI should be performed 24–40 hours after hCG administration. • Natural cycles:• In unmedicated/natural cycles, schedule IUI 1 day after detection of spontaneous LH surge. • Safety cut-offs (multiple pregnancy risk):• Cancel IUI if there are >3 dominant follicles >15 mm on trigger day or estradiol ≥1500 pg/mL due to high multiple pregnancy risk
ESHRE Guideline • Monitoring during COS includes serial transvaginal ultrasound to track follicle count and growth. • Hormonal monitoring (estradiol/progesterone) in addition to ultrasound alone is generally not superior and often not required routinely. • Endometrial thickness may be measured once around trigger day for prognosis but routine multiple endometrial thickness checks are not strongly recommended. Note: Current ESHRE updates (2025) reorganize ovarian stimulation best practices but do not specify exact follicle size thresholds for triggering in IVF/ICSI; clinicians tailor trigger timing based on multi-factorial assessment including follicle cohort size, hormone levels, and patient-specific factors.
Summary • ✔ Follicular tracking guides timing of conception and fertility interventions. ✔ Transvaginal ultrasound is the cornerstone technique. ✔ Guidelines support its use in IUI and IVF monitoring. ✔ Hormone testing and new tech enhance accuracy. • Key takeaway: Accurate tracking increases success and safety of fertility treatments.
Summary • ✔ Trigger follicle size:• ~18–21 mm as primary target for IUI trigger. • ✔ Trigger-IUI interval:• 24–40 hours post-hCG administration. • ✔ When to cancel cycles:• >3 follicles ≥15 mm or estradiol ≥1500 pg/mL. • ✔ Ultrasound scanning schedule:• Baseline day 2–3 → every 1–3 days until target follicle size.
References • Ultrasound role & monitoring basics — Open Access Journals. • National Clinical Practice Guidelines (HSE) for IUI & Fertility. • IVF/ICSI Monitoring Recommendations. • ESHRE Guidelines on Ovarian Stimulation. • Technique & scan scheduling info.