Pelvic Inflammatory Disease
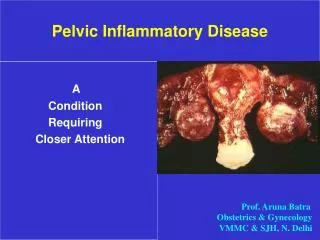
Pelvic Inflammatory Disease. A Condition Requiring Closer Attention. Prof. Aruna Batra Obstetrics & Gynecology VMMC & SJH, N. Delhi. PID: A Neglected Issue. • Low disease awareness

Pelvic Inflammatory Disease
E N D
Presentation Transcript
Pelvic Inflammatory Disease A Condition Requiring Closer Attention Prof. Aruna Batra Obstetrics & Gynecology VMMC & SJH, N. Delhi
PID: A Neglected Issue • Low disease awareness • Sub-optimal management • 50% named correct antibiotic regimen • < 25% examined the sexual partners A National Audit of PID Diagnosis & Management in GP: England and WalesInt. J STD AIDS 2000 Jul;11(7):440-4
Objectives • What is Pelvic Inflammatory Disease? • Why is it important to treat timely? • Causative factors and transmission? • How does the patient present? • Treatment Plan? - Drug therapies - Surgical procedures - Follow up
What is PID ? • Acute/ Chronic clinical syndrome • Inflammation of pelvic structures • Ascending spread of infection from the vagina and endocervix to the endometrium, fallopian tubes, ovaries, &/ or adjoining structures • Upper genital tract infection, salpingitis endometritis, parametritis, tubo-ovarian abscess & pelvic peritonitis
Transmission • • Sexual transmission • via the vagina & cervix • • Gynecological • surgical procedures • • Child birth/ Abortion • • A foreign body inside uterus (IUCD)
Transmission • • Contamination from • other inflamed structures • in abdominal cavity • (appendix, gallbladder) • • Blood-borne transmission • (pelvic TB)
Infective Organisms • • Sexually transmitted - Chlamydia trachomatis • Neisseria gonorrhoeae • • Endogenous Aerobic - Streptococci • Haemophilus • E. coli • • Anaerobes - Bacteroides, Peptostrptococcus • - Bacterial Vaginosis • - Actinomyces israelii • • Mycoplasma hominis, Ureaplasma • • Mycobacterium tuberculosis & bovis
Predisposing Factors • • Frequent sexual encounters, many partners • • Young age, early age at first intercourse • • Exposure immediately prior to menstruation. • • Relative ill-health & poor nutritional status. • • Previously infected tissues (STD/ PID) • • Frequent vaginal douching
Whyis it Important to Treat PID ? • • Systemic upset / Tubo-ovarian abscess • • Chronic Pain (15-20 %)→ Hysterectomy • ● Ectopic pregnancy (6-10 fold) • ● Infertility (Tubal): 20% ~ 2 episodes 40% ~ 3 episodes • ● Recurrence (25%) • ● Male genital disease (25%) • ● Cancer Cervix/ Ovarian Cancer?
Presentation: Acute PID • • Severe pain & tenderness lower abdomen • • Fever, Malaise, vomiting, tachycardia • • Offensive vaginal discharge • • Irregular vaginal bleeding • • B/L adnexal tenderness • • cervical excitation • • Tubo-ovarian mass • • Fitz-Hugh-Curtis Syndrome • Poor sensitivity & specificity • Correct diagnosis : 45 – 70%
Presentation: Chronic PID • • Chronic lower abdominal pain, Backache • • General malaise & fatigue • • Deep dyspareunia, Dysmennorhea • • Intermittent offensive vaginal discharge • • Irregular menstrual periods • • Lower abdominal/ pelvic tenderness • • Bulky, tender uterus • Infertility ( “Silent epidemic” )
PID: Differential Diagnosis • Ectopic Pregnancy • Torsion/ Rupture adnexal mass • Appendicitis • Endometriosis • Cystitis/ pyelonephritis
Laboratory Studies •Pregnancy test • Complete blood count, ESR, CRP • Urinalysis •Gonorrhea, Chlamydia detection (Gram stain/ Cultures / ELISA/ FA/ DNA ) • Tests for TB, syphilis, HIV • Pelvic Ultrasound • Culdocentesis • Laparoscopy
Syndromic Diagnosis of PID Minimum Criteria for Diagnosis (CDC 2002) • • Lower abdominal tenderness on palpation • • Bilateral adnexal tenderness • • Cervical motion tenderness • No other established cause • Negative pregnancy test
Additional Criteria (CDC 2002) • • Oral temperature > 38.3°C (101°F) • • Abnormal cervical / vaginal discharge • • Elevated ESR • • Elevated C-reactive protein • • WBCs on saline micro. of vaginal sec. • • Lab. documentation of cervical infection with N. gonorrhoeae/ C. trachomatis
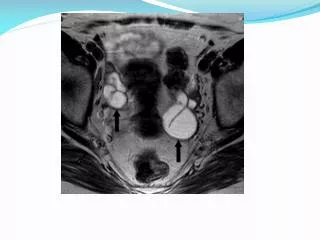
Definitive Criteria (CDC 2002) • Endometrial biopsy with histopathology evidence of endometritis • TVS/ MRI: Thickened fluid filled tubes/ free pelvic fluid / tubo-ovarian complex • Laparoscopic abnormalities consistent with PID
Management Issues • • Inpatient vs. outpatient management ? • • Broad-spectrum antibiotic therapy • without microbiological findings • vs. • Antibiotic treatment adapted to the microbiological agent identified ? • • Oral vs. Parenteral therapy? • • Duration of the treatment ? • • Associated treatment ? • • Prevention of re-infection ?
Criteria for Hospitalization (CDC 2002) • Surgical emergencies not excluded • Severe illness/ nausea/ vomit/ high fever • Tubo-ovarian abscess • Clinical failure of oral anti-microbials • Inability to follow/ tolerate oral regimen • Pregnancy • Immunodeficient (HIV ē low CD4 counts, immunosuppressive therapy)
Antibiotic Therapy Gonorrhea : Cephalosporins, Quinolones Chlamydia: Doxycycline, Erythro-mycin & Quinolones (Not to cephalosporins) Anaerobic organisms: Flagyl, Clindamycin and in some cases to Doxycycline. Beta hemolytic streptococcus and E. Coli Penicillin derivatives, Tetracyclines, and Cephalosporins., E. Coli is most often treated with the penicillins or gentamicin.
Antibiotic Regimens (CDC 2002) Parenteral regimen A Cefoxitin 2 g IV q 6h / cefotetan 2 g IV q 12h + Doxycycline 100 mg PO/IV q12h + Metronidazole or Clindamycin (TO abscess) Parenteral regimen B Clindamycin 900 mg IV q 8h + Gentamicin Loading dose 2 mg/kg IV/IM, maintenance 1.5 mg/kg IV/ IM q 8h
Other 2nd/ 3rd Generation Cephalosporins Ceftizoxime - Cefizox, Cefotaxime - Omnatex, Ceftriaxone - Monocef, Cefoperazone - Magnamycin, Ceftizidime - Fortum
Alternative Parenteral Regimens (CDC 2002) Ofloxacin 400 mg IV q 12 hours or Levofloxacin 500 mg IV once daily WITH OR WITHOUT Metronidazole 500 mg IV q 8 hours or Ampicillin/Sulbactam 3 g IV q 6 hrs PLUS Doxycycline 100 mg orally/ IV q 12 hrs
Outpatient Antibiotic Therapy Regimen A (CDC 2002) Ofloxacin 400 mg twice daily for 14 days or Levofloxacin 500 mg once daily for 14 days WITH OR WITHOUT Metronidazole 500 mg twice daily for 14 days
Outpatient Antibiotic Therapy Regimen B (CDC 2002) Ceftriaxone 250 mg IM once OR Cefoxitin 2 g IM ē probenecid 1 g PO once + Doxycycline 100 mg PO bid for 14 WITH OR WITHOUT Metronidazole 500 mg BD x 14 d
CDC Recommendations • No efficacy data compare parenteral with oral regimens •Clinical experience should guide decisions reg. transition to oral therapy •Until regimens that do not adequately cover anaerobes have been demonstrated to prevent sequelae as successfully as regimens active against these microbes, anaerobic coverage should be provided
When should treatment be stopped ? • Parenteral changed to oral therapy after 72 hrs, if substantial clinical improvement • Continue Oral therapy until clinical & biological signs (leukocytosis, ESR, CRP) disappear or for at least 14 days • If no improvement, additional diagnostic tests/ surgical intervention for pelvic mass/ abscess rupture
Associated treatment Rest at the hospital or at home Sexual abstinence until cure is achieved Anti-inflammatory treatment Dexamethasone 3 tablets of 0.5 mg a day or Non steroidal anti-inflammatory drugs Oestro-progestatives: contraceptive effect + protection of the ovaries against a peritoneal inflammatory reaction + cervical mucus induced by OP has preventive effect against re-infection.
Special Situations Pregnancy - Augmentin or Erythromycin - Hospitalization Concomitant HIV infection - Hospitalization and i.v. antimicrobials - More likely to have pelvic abscesses - Respond more slowly to antimicrobials - Require changes of antibiotics more often - Concomitant Candida and HPV infections
Surgery in PID Indications Acute PID -Ruptured abscess - Failed response to medical treatment - Uncertain diagnosis Chronic PID - Severe, progressive pelvic pain - Repeated exacerbations of PID - Bilateral abscesses / > 8 cm. diameter - Bilateral uretral obstruction
Surgery in PID • Timing of Surgery - No improvement within 24-72 hours - Quiescent (2-3 months after acute stage) • Type of Surgery - Colpotomy - Percutaneus drainage/ aspiration - Exploratory Laparotomy • Extent of Surgery - Conservation if fertility desired - U/L or B/L S.Ophrectomy ē/ š subtotal/ TAH - Drainage of abscess at laporortomy - Identification of ureters
Ruptured Pelvic Abscess ▪ Generalized Septic Peritonitis • ↑ absorption of bacterial endotoxins • ↑ fluid from inflamed peritoneal surfaces • Fluid shift intravascular to interstitial spaces • Hypovolemia, ↓ CO, VC, ↑ PR • ↓ tissue perfusion, ARDS, hyoxemia • Multi-organ system failure Prompt Diagnosis & Treatment
Ruptured Abscess- Management • Pre-Operative • Rapid/ adequate metabolic/hemodynamic preparation • Blood chemistry, CVP monitoring, ABG • X-match blood, IV fluids, aggressive antibiotics • Operative Management • Technical difficulties • Aggressive lavage of peritoneal cavity • Exploration for sub-diaphragmatic collection • Closed suction drain • Post- Operative • Shock, infection, ileus, fluid balance
Follow Up ●Re-screening for Chlamydia & Gonorrhea ● Patient counseling: - Risk of re- infection and sequel. - Sexual counseling - Avoid douching
Management of sex partners • Examination and treatment if they had sexual contact with patients during the 60 days preceding the onset of symptoms in the patients. • Empirical treatment with regimens effective against C. trachomatis and N. gonorrhoeae
Opportunities for Control STD PID Infertility STD Influenced by Interaction of following Environments Genital MicrobialEnvironment Individual BehavioralEnvironment Socio-geographicEnvironment
Prevention • Primary Prevention: • - Sexual counseling: practice safe sex, limit the number of partners, avoid contact with high-risk partners, delay the onset of sexual activity until ≥ 16 years. • - Barrier and Oral contraceptives reduce the risk for developing PID. • Secondary Prevention: • • - Screening for infections in high- risk. • - Rapid diagnosis and effective treatment of STD and lower urinary tract infections. • Tertiary Prevention: • -Early intervention & complete treatment.
Conclusion • ● PID in women - “Silent epidemic” • ● Can have serious consequences. • ● Be aware of limitations of clinical diagnosis. • ● Adequate analgesia and antibiotics. • ● Proper follow up is essential. • ● Treatment of male partner • ● Educational campaigns for young women and health professionals. • ● Prevention by appropriate screening for STD and promotion of condom usage.