Download
1 / 37
370 likes | 601 Views
Why Do This Audit?. Clinical situationCEMD 1997

E N D
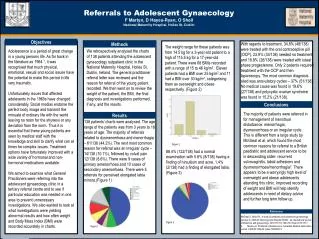
1. Audit of Antenatal Referrals to the Anaesthetist
Dr E A Chubb SpR Anaesthetics
Dr G E W Roberts Consultant Anaesthetist
October 2008
3. OAA /AAGBI Guidelines for Obstetric Anaesthetic Services (2005)
Section 4 : Services and Standards
� Guidelines should be available to obstetricians and midwives on conditions requiring antenatal referral to the anaesthetist.
A system should be in place to ensure that such women are seen and assessed by a senior anaesthetist within a suitable time frame, preferably in early pregnancy�
4. OAA /AAGBI Guidelines for Obstetric Anaesthetic Services (2005) Section 9 : List of recommended protocols
1) Conditions requiring antenatal referral to the anaesthetist
5. NWW Trust guideline for Antenatal Referrals to the Anaesthetist � March 2007 Difficult airway
CVS disease
RS disease
Musculoskeletal
CNS disease
Haematological
Endocrine Renal disease
Hepatic disease
Immune
Transplant patients
Obstetric problems
Previous anaesthetic problems
Medical conditions of note
6. Method Retrospective review of case notes
Cross reference to Trust guidelines
Does the patient have co-morbidity requiring anaesthetic referral?
7. Method Retrospective review of case notes
Cross reference to Trust guidelines
Does the patient have co-morbidity requiring anaesthetic referral?
Was patient referred antenatally?
8. Method Retrospective review of case notes
Cross reference to Trust guidelines
Does the patient have co-morbidity requiring anaesthetic referral?
Was patient referred antenatally?
Was anaesthetic intervention needed?
9. Method Retrospective review of case notes
Cross reference to Trust guidelines
Does the patient have co-morbidity requiring anaesthetic referral?
Was patient referred antenatally?
Was anaesthetic intervention needed?
Any anaesthetic complications?
10. Results
11. Cases requiring referral Jehovah�s Witness
Poorly controlled epilepsy
Antiphospholipid Syndrome
Spina Bifida
12. Cases antenatally referred Jehovah�s Witness
Poorly controlled epilepsy
Antiphospholipid Syndrome
Spina Bifida
13. Cases requiring anaesthetic intervention Jehovah�s Witness
Poorly controlled epilepsy
Antiphospholipid Syndrome
Spina Bifida
14. Results 1 anaesthetic intervention (epidural)
No adverse incidents/outcomes
15. Jehovah�s Witness Issues of blood transfusion
Advance Directives
? Cell salvage
? Blood �fractions� e.g albumin
? Epidural blood patch
Clinicians right to refuse elective treatment
16. Poorly controlled Epilepsy 24 yr old primip
Brittle control since diagnosis
Daily absences , Tonic-clonic seizures at least once a month
Medications : Epilim Chrono 1000mg bd
Ethosuxamide 750mg bd
Under review at the Walton Hospital (last in 12/2006)
17. Poorly controlled Epilepsy Increased risk of : Pre-eclampsia
Antepartum haemorrhage
IUGR
Caesarean section
Seizures triggered by pain,anxiety,excitement
Increased frequency in 45%
Lowered seizure threshold (EFL)
18. Antiphospholipid Syndrome Thrombosis
Increased risk of miscarriage
pre-eclampsia
placental abruption
IUGR
Mother - stroke , MI , valvular lesions (AR)
Treatment involves aspirin , heparin
19. Spina Bifida NTD ~ 1 in 1000
Spina bifida cystica vs. Spina bifida occulta
20. Spina Bifida NTD ~ 1 in 1000
Spina bifida cystica vs. Spina bifida occulta
Spina bifida occulta
<20% incidence � failure of fusion of 1 arch
no external lesion
cord normal
21. Spina Bifida NTD ~ 1 in 1000
Spina bifida cystica vs. Spina bifida occulta
Spina bifida occulta
<20% incidence � failure of fusion of 1 arch
no external lesion
cord normal
Problem: SBO vs. occult spinal dysraphism
22. Spina Bifida Issues: Increase in problematic blocks
Dural puncture
Direct trauma to low lying cord
If patient has : neurological abnormalities
cutaneous manifestation ? tethered
> 1 lamina involved cord
24. Under the Radar Gitelman�s syndrome
Primary renal tubular hypokalaemic metabolic acidosis
K2+
Mg2+
Ca2+
Generalised weakness and muscle cramps
26. The Maths slide 4 out of 144 = 3% needing referral
25% referred
2000 deliveries / year = 60 cases
Based on this audit = 45 cases of special interest not referred a year
27. Is This A Problem? Small numbers
No action in the one referred
Epidural sited in one case once referred in labour
No critical incidents
�First do no harm�
28. Reasons for lack of referral New guideline
Clear lines of referral?
Do Obstetricians know it exists?
ANC
Community clinics
29. Action on this Audit Review guideline
Raise awareness of its existence
copies to respective clinics
Feedback from Obstetric colleagues
High (anaesthetic) risk folder on LW
Re-audit in 6 � 12 months
Audit of cases actually referred
30. Cases Referred Aortic / pulmonary valve replacement
Morbid obesity + asthma
Extreme needle phobia
Hemiglossectomy
Exercise � induced anaphylaxis
31. And One That Wasn�t 01:40 � 2cm dilated , request for epidural
32. And One That Wasn�t 01:40 � 2cm dilated , request for epidural
Tetralogy of Fallot � corrected aged 8
seen in ANC
Cardiology opinion
33. Cardiology Opinion �As I mentioned in my previous letter, I don�t expect too much of a problem during delivery.
She will obviously require antibiotic prophylaxis and also need high flow O2 during delivery�
34. Echocardiogram Normal LV + function
Normal Aortic / Mitral valves
Dilated RV
Moderate PR / TR
? Pulmonary hypertension
( Echo 2004 � PAP of 35mmHg)
35. Summary Antenatal consultation achieves many goals
Anaesthetic involvement in high risk cases desirable ( OAA / AAGBI)
( CEMD / CEMACH )
36. Summary Antenatal consultation achieves many goals
Anaesthetic involvement in high risk cases desirable ( OAA / AAGBI)
( CEMD / CEMACH )
THANKYOU FOR YOUR ATTENTION
37. References Why Mothers Die 1997 � 1999 : CEMD 2001
Saving Mothers Lives 2003 � 2005 : CEMACH 2007
Guidelines for Obstetric Anaesthetic Services (revised edition):OAA/AAGBI 2005
Obstetric Anaesthesia and Uncommon Disorders :Gambling et al, 2008
Spina Bifida, tethered cord and regional anaesthesia : Ali , Anaesthesia 2005
Anaesthetic management of parturients with antiphospholipid syndrome; a review
of 27 cases : CJ Ralph, IJOA October 1999
C-281 Guideline for Antenatal Referrals to the Anaesthetist: NWW NHS Trust 2007