Download

1 / 7
0 likes | 12 Views
our Indian Research Journal of Pharmacy and Science (IRJPS) is a multidisciplinary, peer-reviewed, open-access journal that publishes research across various scientific fields, primarily focusing on pharmaceutical sciences, biotechnology, and life sciences. Published quarterly by the Phytotherapy Research Group in Guwahati, India, IRJPS emphasizes research collaboration within the pharmaceutical and healthcare industries.

E N D
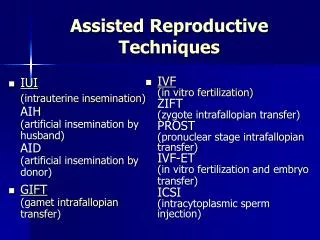
Archana et al. International Research Journal of Pharmacy, 2023, 14:02:16-22. Research Article INTERNATIONAL RESEARCH JOURNAL OF PHARMACY www.irjponline.com ISSN 2230-8407 [LINKING] COMPARATIVE ANALYSIS OF THE RESULTS OF NON-ART CONCEPTION AND PRETERM NEONATES DELIVERED TECHNOLOGIES Dr. Archana USING ASSISTED REPRODUCTIVE Assistant Professor, Department of Obstetrics & Gynaecology, Himalayan Institute of Medical College and Hospital, Dehradun, Uttarakhand Email:- sharmaarchana1978@gmail.com How to cite: Archana. Comparative analysis of the results of non-art conception and preterm neonates delivered using assisted reproductive technologies. International Research Journal of Pharmacy, 2023, 14:02:16-22. DOI: 10.56802/2230-8407.1303207 ================================================================================== ABSTRACT Background: Studies on the outcomes of extremely preterm neonates delivered with assisted reproductive technologies are rare and have produced inconsistent findings in the literature. Aim: to evaluate in comparison the outcomes of non-ART conception and preterm neonates delivered using assisted reproductive technologies (ARTs). Methods: The extremely preterm newborns who were hospitalised to the institute's neonatal unit throughout the research period and born between 26 and 31 weeks gestation were evaluated in this study. The composite adverse outcome of mortality was the main outcome that was evaluated, along with any other significant morbidities such as ROP (retinopathy of prematurity), BPD (bronchopulmonary dysplasia) at 36 weeks, grade II or higher PVL (periventricular leukomalacia), and IVH (intraventricular haemorrhage) grade III or higher that required medical attention. Results: 380 newborns were evaluated for the research; 127 were in the ART group and 258 were in the non-ART group. The neonates were matched for age, gender, and small for gestational age (SGA). With OR (95% CI) of 0.84 (0.53-1.34), ROP needing treatment of 0.47 (0.12-1.69), BPD of 1.16 (0.35-3.74), death of 0.91 (0.51-162), and other morbidities, neonates in the ART group had comparable rates of composite unfavourable outcomes. Conclusion: In comparison to neonates delivered using non-assisted reproductive procedures, the current study's conclusions indicate that extremely preterm newborns born by assisted reproductive techniques do not have an increased risk of unfavourable neonatal outcomes. Keywords: very preterm neonates, ART (assisted reproductive techniques), small for gestational age, non-ART INTRODUCTION Assisted reproductive technologies (ART) have been connected to an increased risk of low birthweight, neonatal problems, and spontaneous preterm birth. According to the World Health Organization's definition, assisted reproductive methods encompass all in vitro procedures and treatments involving the manipulation of human sperm, oocytes, or embryos in order to produce pregnancy.The World Health Organization's 1,2 definition excludes and does not take artificial insemination into consideration. The cryopreservation of embryos or gametes, aberrant methylation, 16
Archana et al. International Research Journal of Pharmacy, 2023, 14:02:16-22. in vitro modification, mother age, and epigenetic diseases can all have a significant impact on the results of assisted reproductive procedures. These variables that control the results of assisted reproductive methods may also have a major role in the unfavourable results of these methods.3,4 In evaluating the results of assisted reproductive procedures, it is critical to comprehend this pathological plausibility with regard to the inclusion of newborns and babies in the group.5 There are few, conflicting studies evaluating the outcomes for extremely preterm newborns delivered using assisted reproductive technologies in middle-class and low- income countries.6,7 The World Health Organization's criteria, which evaluated the primary congenital defects that may influence the outcomes independently, is not strictly followed by the bulk of the literature data now in existence.8. The World Health Organization's definition of extremely preterm neonates is used in this study to evaluate the outcomes for those babies born using assisted reproductive technologies. The purpose of the current study was to compare the outcomes of preterm neonates delivered with assisted reproductive technologies (ARTs) against non-ART conception. MATERIAL AND METHODS The goal of the current retrospective clinical investigation was to evaluate the outcomes of preterm neonates delivered with assisted reproductive technologies (ARTs) vs those born without ARTs. The study evaluated the data from the Institute's newborn intensive care unit (NICU) in hindsight. Data were collected sequentially for every extremely preterm newborn that was found in the Institute's old files. The study's exclusion criteria included newborns born before 26 weeks of pregnancy, those weighing less than 600 grammes at birth, those who were not receiving active therapy, those who were sent to another centre before their due date, and those with significant congenital defects. Since these topics weren't handled and cared for at the Institute, they were eliminated. Infants born with IVF (in vitro fertilisation) and ICSI (intracytoplasmic sperm injection) were classified as part of the ART group, according the World Health Organization's classification.The non-ART group included nine newborns born by ovulation inducement (OI) and intrauterine insemination (UIU). After the day of fertilisation, gestational age was determined by retrieving the oocytes, waiting an extra 14 days, doing a first trimester ultrasound, and then using a fresh Ballard score postnatally for confirmation. According to the Fenton 2013 growth chart, birthweights fewer than the third and tenth centiles for gestational age, respectively, were considered severe SGA (small for gestational age) and SGA. The requirement for any kind of respiratory assistance at 36 weeks PMA (post-menstrual age) was the criteria for BPD (bronchopulmonary dysplasia). Regarding the evaluation of ROP (retinopathy of prematurity), PVL (periventricular leukomalacia), and IVH (intraventricular haemorrhage), respectively, ETROP guidelines, DeVries classification, and Volpe classification were adhered to. According to Fenton growth charts, discharge weight <10th centile for discharge PMA and sex was considered extrauterine growth restriction, or EUGR. Comparing the composite adverse outcome—defined as in-hospital death or one or more serious morbidities, such as ROP requiring treatment, BPD, PVL of grade 2 or higher, and IVH of grade 3 or higher—was the study's main goal. For the purpose of evaluating descriptive measures, the collected data were statistically analysed using SPSS (Statistical Package for the Social Sciences) software version 16.0 (SPSS Inc., Chicago, USA). The findings were presented as percentages, frequency, mean, and standard deviation. When the p- value was less than 0.05, it was deemed statistically significant. The Chi-square test was used to determine the research parameters' significance on the categorical scale. In cases where ANOVA showed significant results, post-hoc Turkey analysis was done. RESULTS The goal of the current retrospective clinical investigation was to evaluate the outcomes of preterm neonates delivered with assisted reproductive technologies (ARTs) vs those born without ARTs. A total of 380 newborns were evaluated 17
Archana et al. International Research Journal of Pharmacy, 2023, 14:02:16-22. for the trial; 127 of them were matched for age, gender, and SGA (small for gestational age) and 258 of them were in the non-ART group. With p<0.001, the mean maternal age in the ART group was much greater—32.71±4.41 years— than in the non-ART group, which was 28.84±4.13. With p=0.25, the gestational ages of the two groups were similar. In the ART group, the prevalence of gestational diabetes was considerably higher (p=0.003). With p=0.25, PIH was substantially similar between the ART and non-ART groups. With p<0.001, the ART group's primipara, primigravida, and multifetal gestation rates were considerably greater than those of the non-ART group. Table 1 indicates that the following characteristics of the ART and non-ART groups were statistically comparable: no antenatal steroid need, severe SGA, SGA, male gender, birthweight, resuscitation at birth, APGAR <7 at 5 minutes, caesarean delivery rate, PPROM, and chorioamnionitis. The corresponding p-values were 0.7, 0.71, 0.63, 0.3, 0.84, 0.71, 0.91, 0.4, and 0.52. ROP requiring treatment was observed in 1.57% (n=2) subjects from the ART group and 3.48% (n=9) subjects from the non-ART group, demonstrating statistical non-significance with p=0.24. When major comorbidities and mortality were assessed in infants born from ART and non-ART, the mortality in the ART and non-ART groups were 14.17% (n=18) and 10.46% (n=27), respectively. A statistically non-significant p-value of 0.36 indicated that PVL grade ≥2 was observed in 3.14% (n = 4) and 1.93% (n = 5) of participants from the ART and non-ART groups, respectively. A statistically non-significant p-value of 0.34 indicated that IVH grade ≥3 was seen in 6.29% (n=8) and 4.26% (n=11) of participants from the ART and non-ART groups, respectively. At 35 weeks PMA, 3.14% (n=4) and 2.32% (n=6) of the individuals in the ART and non-ART groups, respectively, had BPD that required respiratory assistance; this difference was statistically not significant (p=0.76). Table 2 shows that composite unfavourable outcomes from any of the aforementioned five were observed in 22.04% (n=28) and 22.86% (n=59) of participants from the ART and non-ART groups, respectively. This difference was statistically not significant at p=0.51. According to the study's findings, there were 22.83% (n=29) and 28.29% (n=73) of participants from the ART and non-ART groups, respectively, who had any grade IVH for baby outcomes. These findings were statistically not significant, with a p- value of 0.313. In the ART and non-ART groups, culture-positive sepsis was observed in 24.40% (n=31) and 26.74% (n=69) of participants, respectively. These findings were statistically non-significant with p=0.07. 7.08% (n=9) and 8.13% (n=21) of the individuals in the ART and non-ART groups, respectively, had NEC stage 2A or higher; these differences were not statistically significant (p=0.16). In the ART and non-ART groups, PDA surgical ligation was observed in 2.36% (n=3) and 0.77% (n=2) of the individuals, respectively. This difference was not statistically significant (p=0.1). >28 days oxygen need was observed in 17.32% (n=22) and 15.11% (n=39) subjects from ART and non-ART groups respectively, which was non-significant with 0.63. Hs-PDA requiring treatment was needed in 25.98% (n=33) and 25.81% (n=66) subjects from ART and non-ART groups, respectively, which was significantly higher in the ART group with p=0.03. Invasive respiratory support duration was comparable in ART and non-ART groups with p=0.44 (Table 3). With p=0.94, it was shown that the length of respiratory support was similar in the ART and non-ART groups. Moreover, surfactant was observed in similar amounts in the ART and non-ART groups (p= 0.08). Comparable percentages of RDS and EUGR were seen in the ART and non-ART groups (p=0.12 and p=0.67, respectively). At discharge, the newborns' weights in the ART and non-ART groups were, respectively, 1522 and 1480 grammes, which was statistically not significant (p=0.37). Discharge PMA (weeks) was seen in 17.38% (n=17) of participants in the ART group and 6.58% (n=17) of subjects in the non-ART group, respectively (p=0.54). In the ART and non-ART groups, respectively, 8.66% (n=11) and 12.40% (n=32) of the individuals had any ROP; this difference was statistically not significant, with p=0.18 (Table 3). DISCUSSION A total of 380 newborns were evaluated in this study; 127 of them were in the ART group and 258 of them were in the non-ART group. The neonates were matched for age, gender, and gestational age (SGA). With p<0.001, the mean maternal age in the ART group was much greater—32.71±4.41 years—than in the non-ART group, which was 28.84±4.13. With p=0.25, gestational age was similar across the two groups. With p=0.003, the ART group exhibited 18
Archana et al. International Research Journal of Pharmacy, 2023, 14:02:16-22. a noticeably higher frequency of gestational diabetes. With p=0.25, PIH was substantially similar between the ART and non-ART groups. With a p-value of less than 0.001, the ART group saw substantially greater rates of multifetal gestation, primipara, and primigravida than the non-ART group. The ART and non-ART groups showed statistically comparable rates of chorioamnionitis, PPROM, antenatal steroid use, severe SGA, male gender, birthweight, resuscitation at birth, APGAR <7 at 5 minutes, caesarean delivery rate, and PPROM, with corresponding p-values of 0.7, 0.71, 0.63, 0.3, 0.84, 0.91, 0.4, and 0.52. The present study's results bore similarities to those of studies conducted by Anne RP et al. (10 in 2022) and Gao L et al. (11 in 2019), in which the authors evaluated newborns whose mothers had similar demographic data. When the primary comorbidities and mortality of infants born into ART and non-ART groups were compared, it was found that the mortality in the ART group was 14.17% (n=18) and the non-ART group was 10.46% (n=27), respectively. These results were statistically non-significant with p=0.6. 1.57% (n = 2) of the ART group's participants and 3.48% (n = 9) of the non-ART group's subjects had ROP that required treatment; the statistical non-significance was shown with p = 0.24. A statistically non-significant p-value of 0.36 indicated that PVL grade ≥2 was seen in 3.14% (n=4) and 1.93% (n=5) of participants from the ART and non- ART groups, respectively. A statistically non-significant p-value of 0.34 indicated that IVH grade ≥3 was observed in 6.29% (n = 8) and 4.26% (n = 11) of participants from the ART and non-ART groups, respectively. At 35 weeks PMA, 3.14% (n=4) and 2.32% (n=6) of the individuals in the ART and non-ART groups, respectively, had BPD that required respiratory assistance; this difference was statistically not significant (p=0.76). In the ART and non-ART groups, composite unfavourable outcomes from any of the above five were observed in 22.04% (n=28) and 22.86% (n=59) of the participants, respectively. This difference was statistically not significant (p=0.51). The findings aligned with the research conducted by Ahmad KA et al. in 2019 and Picaud JC et al. in 2012, wherein the authors observed similar major comorbidities and death rates in children born on ART and non-ART. According to the results for babies born into ART and non-ART groups, there were 22.83% (n=29) and 28.29% (n=73) of participants from the ART and non-ART groups, respectively, who had any grade IVH. This difference was statistically not significant (p=0.313). In the ART and non-ART groups, culture-positive sepsis was observed in 24.40% (n = 31) and 26.74% (n = 69) of participants, respectively. These findings were statistically non-significant with p = 0.07. 7.08% (n=9) and 8.13% (n=21) of the individuals in the ART and non-ART groups, respectively, had NEC stage 2A or higher; these differences were not statistically significant (p=0.16). In the ART and non-ART groups, PDA surgical ligation was observed in 2.36% (n=3) and 0.77% (n=2) of the individuals, respectively. This difference was not statistically significant (p=0.1). The percentage of participants from the ART and non-ART groups who required therapy for Hs-PDA was 25.98% (n=33) and 25.81% (n=66), respectively. The ART group had a substantially higher rate of Hs-PDA-requiring treatment (p=0.03).The 28-day oxygen requirement was seen in 17.32% (n = 22) and 15.11% (n = 39) of participants in the ART and non-ART groups, respectively. The significance level was 0.63. The duration of invasive respiratory assistance did not differ between the ART and non-ART groups (p=0.44). These results were consistent with the findings of Heo JS et al.14 and Messerschmidt A et al.15, whose authors found similar outcomes in children born from ART and non-ART in their respective investigations. According to the study's findings, the length of respiratory assistance was similar for both the ART and non-ART groups (p=0.94). Moreover, surfactant was observed in similar amounts in the ART and non-ART groups (p= 0.08). Comparable percentages of RDS and EUGR were seen in the ART and non-ART groups (p=0.12 and p=0.67, respectively). At discharge, the newborns' weights in the ART and non-ART groups were, respectively, 1522 and 1480 grammes, which was statistically not significant (p=0.37). Discharge PMA (weeks) was seen in 17.38% (n=17) of participants in the ART group and 6.58% (n=17) of subjects in the non-ART group, respectively (p=0.54). In the ART and non-ART groups, respectively, 8.66% (n=11) and 12.40% (n=32) of the participants had any ROP; this difference was statistically not significant (p=0.18). 19
Archana et al. International Research Journal of Pharmacy, 2023, 14:02:16-22. These results were consistent with those of Fineman DC et al.16 in 2021 and Hogberg U et al.17 in 2007, whose authors observed comparable outcomes in extremely preterm children delivered from ART in their separate investigations. CONCLUSION Taking into account its limitations, the current study finds that neonates delivered extremely preterm by assisted reproductive procedures do not have a greater risk of poor neonatal outcomes than neonates born via non-assisted reproductive techniques. For a conclusive result, however, further longitudinal studies with a greater number of newborns in various geographic locations are necessary. REFERENCES 1.Pandey S, Shetty A, Hamilton M, et al. Obstetric and perinatal outcomes in singleton pregnancies resulting from IVF/ICSI: A systematic review and meta-analysis. Hum Reprod Update. 2012;18:485-503. 2.Turker G, Doger E, Arýsoy AE, et al. The effect of IVF pregnancies on mortality and morbidity in the tertiary unit. Ital J Pediatr. 2013;39:17. 3.Cavoretto P, Candiani M, Giorgione V, et al. Risk of spontaneous preterm birth in singleton pregnancies conceived after IVF/ICSI treatment: A meta-analysis of cohort studies. Ultrasound Obstet Gynecol. 2018;51:43-53. 4.Zegers-Hochschild F, Adamson GD, de Mouzon J, et al. The International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised the glossary on ART terminology, in 2009. Hum Reprod. 2009;24:2683-7 5.Corchia C, Da Frè M, Di Lallo D, et al. Mortality and major morbidities in very preterm infants born from assisted conception or naturally conceived: results of the area-based ACTION study. BMC Pregnancy Childbirth. 2014;14:307. 6.Chiarelli L, Mirea L, Yang J, Lee SK, Shah PS, Canadian Neonatal Network. Neonatal outcomes in very preterm singleton infants conceived using assisted reproductive technologies. Am J Perinatol. 2015;32:515- 22 7.Schimmel MS, Hammerman C, Lusky A, Reichman B. Very low-birth-weight-infants conceived by in vitro fertilization are not at higher risk for mortality and morbidity: a population-based study. Fertil Steril. 2006;85:907-12 8.Schimmel MS, Hammerman C, Lusky A, Reichman B. Very low-birth-weight-infants conceived by in vitro fertilization are not at higher risk for mortality and morbidity: a population-based study. Fertil Steril. 2006;85:907-12 9.Tarin JJ, García Pérez MA, Cano A. Assisted reproductive technology results: Why are live birth percentages so low? Mol Reprod Dev. 2014;81:568-83. 10.Anne RP, Vardhelli V, Oleti TP, et al. Propensity-matched comparison of very preterm small-and appropriate- for gestational-age neonates. Indian J Pediatr. 2022;89:59-66 11.Gao L, Shao W, Li N, et al. The risk of retinopathy of prematurity in the infants following assisted reproductive technology: A meta-analysis. Biomed Res Int. 2019;20:95730. 12.Ahmad KA, Bennett MM, Rayburn P, et al. Outcomes of preterm infants conceived with in vitro fertilization. J Perinatol. 2019;39:717-22. 13.Picaud JC, Chalies S, Combes C, et al. Neonatal mortality and morbidity in preterm infants born from assisted reproductive technologies. Acta Paediatr. 2012;101:846-51. 14.Heo JS, Lee HJ, Lee MH, Choi CW. Comparison of neonatal outcomes of very low birth weight infants by mode of conception: in vitro fertilization versus natural pregnancy. Fertil Steril. 2019;111:962-70. 15.Messerschmidt A, Olischar M, Birnbacher R, et al. Perinatal outcome of preterm infants < 1500g after IVF pregnancies compared with natural conception. Arch Dis Child Fetal Neonatal Ed. 2010;95:F225-9. 16.Fineman DC, Keller RL, Maltepe E, Rinaudo PF, Steurer MA. Outcomes of very preterm infants conceived with assisted reproductive Technologies. J Pediatr 2021;236:47-53.e1. 20
Archana et al. International Research Journal of Pharmacy, 2023, 14:02:16-22. 17.Hogberg U, Holmgren PA. Infant mortality of very preterm infants by € mode of delivery, institutional policies and maternal diagnosis. Acta Obstet Gynecol Scand 2007;86:693-700. S. No Characteristics ART n=127 32.71±4.41 29.3±1.64 26 56 93 116 78 5 19 1 18 66 1175.79±310.1 33 14 108 42 11 Non-ART n=258 28.84±4.13 29.4±1.51 31 101 64 164 121 11 53 3 32 124 1170.83±271.6 69 28 206 78 21 p-value % % 1. 2. 3. 4. 5. 6. 7. 8. 9. 10.Severe SGA 11.SGA 12.Male gender 13.Birthweight (grams) 14.Resuscitation at birth 15.APGAR <7 at 5 min 16.Cesarean delivery 17.PPROM 18.Chorioamnionitis Table 1:Characteristics of study neonates born in two groups of ART and non-ART Maternal age (years) Gestational age (weeks) Gestational diabetes PIH Multifetal gestational Primipara Primigravida No antenatal steroids Doppler abnormalities <0.001 0.25 0.003 0.25 <0.001 <0.001 <0.001 0.7 0.04 0.71 0.63 0.3 0.84 0.71 0.91 0.4 0.52 1.0 20.47 44.09 73.22 91.33 61.41 3.93 14.96 0.78 14.17 51.96 12.01 39.14 24.80 63.56 46.89 4.26 20.54 1.16 12.40 48.06 25.98 11.02 85.03 33.07 8.66 26.74 10.85 79.84 30.23 8.13 S. No Outcomes ART n=127 18 2 4 8 4 Non-ART n=258 27 9 5 11 6 p-value % 14.17 1.57 3.14 6.29 3.14 % 10.46 3.48 1.93 4.26 2.32 1. 2. 3. 4. 5. Mortality ROP needing treatment PVL grade ≥2 IVH grade ≥3 BPD (respiratory support at 35- weeks PMA) Composite adverse outcome (any of the above 5) Table 2: Major morbidities and mortality in infants born from ART and non-ART 0.6 0.24 0.36 0.34 0.76 6. 28 22.04 59 22.86 0.51 S. No Outcomes ART n=127 29 31 9 3 33 22 0 (0-2) Non-ART n=258 73 69 21 2 66 39 0 (0-2) p-value % 22.83 24.40 7.08 2.36 25.98 17.32 % 28.29 26.74 8.13 0.77 25.81 15.11 1.Any grade IVH 2.Culture positive sepsis 3.NEC stage 2A or more 4.PDA-surgical ligation 5.Hs-PDA requiring treatment 6.>28 days oxygen need 7.Respiratory (Invasive) 0.313 0.07 0.16 0.1 0.03 0.63 0.44 support duration 21
Archana et al. International Research Journal of Pharmacy, 2023, 14:02:16-22. 8.Respiratory (total) 9.Surfactant 10.RDS 11.EUGR 12.Discharge weight (grams) 13.Discharge PMA (weeks) 14.Any ROP 6 (2-16) 7 (3-15) 0.94 support duration 82 86 109 1522 (1422-1662) 17 11 64.56 67.71 85.82 165 174 164 1480 (1420-1620) 17 32 63.95 67.44 63.56 0.08 0.12 0.67 0.37 0.54 0.18 13.38 8.66 6.58 12.40 Table 3: Outcomes in infants born from ART and non-ART 22