Download
1 / 23
230 likes | 1.32k Views
The First Heart Sound (S 1 ) Chapter 7. Ara G. Tilkian, MD, FACC Instructor Patricia L. Thomas, MBA, RCIS. Outline. Components of S 1 How to recognize S 1 at Rapid Heart Rate Physiological Splitting of S 1 Differential Diagnosis S 1 as a Single Sound

E N D
The First Heart Sound (S1)Chapter 7 Ara G. Tilkian, MD, FACC Instructor Patricia L. Thomas, MBA, RCIS
Outline • Components of S1 • How to recognize S1 at Rapid Heart Rate • Physiological Splitting of S1 • Differential Diagnosis • S1 as a Single Sound • Factors Influencing the Intensity of S1
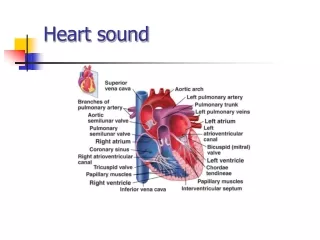
Components of S1 • Marks the mitral (M1)and tricuspid (T1) closure • Loudest heart sound • High frequency components • Vibrations set up in the valve cusps, chordae, papillary muscles and ventricular walls before aortic ejection
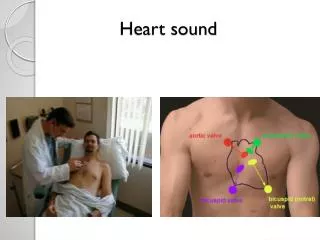
Where to Listen • Listen with the diaphragm & bell of the stethoscope at the apex & 4th left intercostal space
How to Recognize S1 at Rapid Heart Rates • During Auscultation • Slow Heart Rates • Defines the onset of systole which is of shorter duration than diastole • Rapid Heart Rates > 130 b/m • Palpate the Carotid artery: S1 precedes the palpable arterial upstroke • S2 immediately follows this pulse
Differential Diagnosis • Sounds of the Cardiac Cycle In Perspective • Pathological Splitting of S1 • The S4-S1 Combination • S1 Followed by an Ejection Sound • The Presystolic Murmur-S1 Combination
Factors Influencing the Intensity of S1 • Any condition that increases the force of ventricular contraction • Shortens, the PR interval • Brings the heart closer to the chest wall makes S1 louder (loud in children and young adults) • When heart rate is normal, a loud S1 should alert the examiner of a possible short PR interval. • Ventricular Contractility • Pathological alteration of the cardiovascular system
Ventricular Contractility • Influence by the contractility of the Left Ventricle than by the Right Ventricle • Enhanced Contractility • S1 is accentuated (anemia, fever, pregnancy, exercise, anxiety) • Poor Contractility • Decrease in the rate of pressure rise in the left ventricle, the first sound softens. (MI, cardiomypathies, shock)
The PR Interval • Reflects AV conduction time • The time between atrial and ventricular contraction • The shorter the PR interval, the louder the first heart sound (mitral valve leaflets are wide open and deep within the ventricle when contraction begins causing the leaflets to close forcefully. • The longer the PR interval, the softer the first sound • The PR interval directly influences the position of valve leaflets at the onset of ventricular systole
Mitral Stenosis • Mobile mitral cusp, one of the first and most consistent diagnostic clues is a typically loud and slapping heart sound. • The loud S1 of mitral stenosis is caused by the closure of the mitral valve occurring on the steep upslope of the LV pressure curve during isometric contraction. • Short PR interval
Aortic Insufficiency • S1 is diminished or absent in patients • Mitral valve may be prematurely closed when systole begins because of a long PR interval or high Lvedp • Pressures within the aorta a ventricle approach each other during diastole, isovolumic systole is either short or absent, causing a softening of S1
Mitral Regurgitation • S1 absent or weak • Valve leaflets may fail to seal the AV opening during ventricular systole because of structural defects or widening of the valve ring. • Dissipation of LV pressure and the LA • Decrease in the rate of rise of LV pressure weakens the intensity of S1
The heart has been sectioned to reveal the mitral valve as seen from above in the left atrium. The mitral valve demonstrates the typical "fish mouth" shape with chronic,
Left Atrial Myxoma • S1 is loud in patients with mobile myxoma of the LA because of a delay in mitral valve closure • Echocardiography can provide a definitive diagnosis • Mechanism is similar to a short PR interval when the mitral leaflets are widely opened immediately before the onset of ventricular systole
THE ENDOFCHAPTER 7 Tilkian, Ara MD Understanding Heart Sounds and Murmurs, Fourth Edition, W.B. Sunders Company. 2002, pp. 58-71.