Download
1 / 52
1.02k likes | 4.23k Views
Non-GC septic arthritis. Host. Young healthy adults. Young children, elderly, ... prosthetic joints, chronic arthritis. 40% have pre-existing joint ...

E N D
1. SEPTIC ARTHRITIS
Victoria K. Shanmugam, MD Georgetown University Hospital
2. CASE
A 30 year Texan businessman, visiting London Presents December 20th 2002 with headache, pustular skin rash, photophobia, stiff neck
3. Lumbar Puncture
4. But what about my knee?
The following morning on rounds the patient asks �but what about my knee� Attending lifts the sheets to reveal swollen R knee
5. But what about my knee?
The following morning on rounds the patient asks �but what about my knee� Attending lifts the sheets to reveal swollen R knee WHAT IS THE DIAGNOSIS?
6. Disseminated Gonococcal Infection
1-3 % of patients with GC 1 day -3 weeks after sexual encounter Genital infection may be asymptomatic Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients. Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients.
7. Disseminated Gonococcal Infection
1-3 % of patients with GC 1 day -3 weeks after sexual encounter Genital infection may be asymptomatic Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients. Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients.
8. Disseminated Gonococcal Infection
1-3 % of patients with GC 1 day -3 weeks after sexual encounter Genital infection may be asymptomatic Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients. Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients.
9. Disseminated Gonococcal Infection
1-3 % of patients with GC 1 day -3 weeks after sexual encounter Genital infection may be asymptomatic Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients. Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients.
10. Disseminated Gonococcal Infection
1-3 % of patients with GC 1 day -3 weeks after sexual encounter Genital infection may be asymptomatic Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients. Genitourinary isolation rate is 80% Note that organism is killed by exposure to cold Note PCR of synovial fluid may be positive in these patients.
11. Risk factors for GC
Women > Men 3: 1 Recent menses � change in pH around cervix Pregnancy or immediate post-partum Congenital or acquired complement deficiencies C6, C7, C8 Check CH50 Asplenia In men more common if homo/bisexual Virulence factors Serotype Ia Auxotype AHU Strains that fail to express outer membrane protein II Certain strains of GC possess virulence and growth factors which increase risk of dissemination. Serotype 1A � outer membrane surface protein which increases its virulence Strains requiring arginine, hypoxanthine and uracil for growth (Auxotype AHU) Strains that fail to express outer membrane protein II (form transparent rather than opaque colonies) Usually sensitive to penicillin, though some penicillinase producing strains can also cause DGI Certain strains of GC possess virulence and growth factors which increase risk of dissemination. Serotype 1A � outer membrane surface protein which increases its virulence Strains requiring arginine, hypoxanthine and uracil for growth (Auxotype AHU) Strains that fail to express outer membrane protein II (form transparent rather than opaque colonies) Usually sensitive to penicillin, though some penicillinase producing strains can also cause DGI
12. Treatment
Daily drainage if purulent arthritis Antibiotics: Ceftriaxone 1g IV or IM q 24 hours for 10-14 days Switch to Cefuroxime 500mg bid as outpatient Quinolone resistant strains in Hawaii and California Simultaneously treat for Chlamydia: Doxycycline 100mg bid (or erythromycin if pregnant) Asymptomatic partner: Ceftriaxone 125mg IM and doxycycline 100mg bid x7d Test for syphilis and HIV
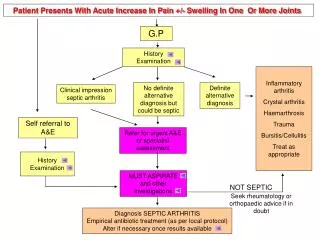
13. Evaluation of a patient with joint swelling
Distribution: Mono/oligo/polyarthritis Small or large joints Systemic symptoms Fevers, chills Risk factors Chronic diseases CRF, DM, HIV, IVDA Exposures/sexual/Lyme DDX: RA/SLE Gout /pseudogout Reactive arthritis
14. CASE
An 85 year old female presents with fever and obtundation. In the ER her mental status improves with IV fluids. Urinalysis is dirty and she is commenced on antibiotics for presumed UTI. 2 days into the hospital admission she develops bilateral shoulder pain, pain, swelling and erythema of the R 3rd PIP, the L wrist and the R ankle. She has severe pain on moving the joints which are exquisitely tender to palpation
15. Ask the audience What do you do next?
The diagnosis is gout give IV colchicine The diagnosis is pseudogout give IM steroids The patient has gram negative septic arthritis from her UTI give ceftazidime Order an echocardiogram Send Lyme serologies
16. ISSUES TO CONSIDER
MANAGEMENT OF SEPTIC ARTHRITIS Risk factors and typical presentation Which joints and bacteria are most involved Special situations How to aspirate a joint and what should the fluid be sent for Choice of empiric antibiotics DDX: What other pathologies should be considered
17. PRESENTATION
Abrupt onset of pain/swelling of one joint Usually patient has other co-morbidities Fever >38 in 40-90% Rigors in 20-60%
18. Just as it takes two to make a quarrel, it takes two to make a disease, the microbe and it�s host�
70% spread hematogenously. Not all septicemic patients develop septic arthritis. Some patients seed joints without signs of bacteremia Only 0.5% of patients with pneumococcal bacteremia Polyarticular septic arthritis consider endocarditis IVDA Staph. aureus, enterococcus or streptococci 20% of septic arthritis is iatrogenic Post arthroscopy or arthrocentesis Risk of infection after arthrocentesis <1% Sternoclavicular joint during line insertion Morgan, DS et al., Epidemiol Infect 1996; 22: 783 There are unique features of the host and the bug that allow septic arthritis to developThere are unique features of the host and the bug that allow septic arthritis to develop
19. What is the diagnosis
An 85 year old female presents with fever and obtundation. In the ER her mental status improves with IV fluids. Urinalysis is dirty and she is commenced on antibiotics for presumed UTI. 2 days into the hospital admission she develops bilateral shoulder pain, pain, swelling and erythema of the R 3rd PIP, the L wrist and the R ankle. She has severe pain on moving the joints which are exquisitely tender to palpation
20. CLINICAL COURSE
Aspirated shoulder and PIP: Gram positive cocci Urine culture: Gram positive cocci
21. What should you do?
The diagnosis is Gout give IV colchicine The diagnosis is pseudogout give IM steroids The patient has gram negative septic arthritis from her UTI give ceftazidime Order an echocardiogram Send Lyme serologies
22. CLINICAL COURSE
Aspirated shoulder and PIP: Gram positive cocci Urine culture: Gram positive cocci Echocardiogram: Vegetation on mitral valve DIAGNOSIS: Endocarditis
23. Risk Factors
Impaired host defense Malignancy, elderly or children, DM, HIV, Cirrhosis, CRF, glucocorticoids, chemo. Penetration Injection drug use, puncture wounds, invasive procedures Sternoclavicular joint during line insertion Septic hip due to ruptured diverticulum Joint damage prosthetic joints, chronic arthritis 40% have pre-existing joint disease usually RA or OA, but can be gout, pseudogout, Charcot�s HIV positive more likely to have opportunistic organisms Kaandorp, CJE et al. Arthritis Rheum 2000; 30: 147 154 patients with bacterial arthritis 40% had underlying joint disease154 patients with bacterial arthritis 40% had underlying joint disease
24. Which joints and which organisms?
25. Which joints and which organisms?
Staph aureus has a collagen adhesion factor which allows it to localize to joints. The presence of the gene for this factor (CNA) is a virulence factor contributing to joint localizationStaph aureus has a collagen adhesion factor which allows it to localize to joints. The presence of the gene for this factor (CNA) is a virulence factor contributing to joint localization
26. Special situations
27. Special situations
28. Special situations
29. Special situations
30. Special situations
31. How do I aspirate a joint?
32. How do I aspirate a joint?
33. How do I aspirate a joint?
Procedures Required for Certification in Internal Medicine For certification in internal medicine, the ABIM requires that candidates must be judged competent by their program directors in: A. performing the following procedures; understanding their indications, limitations, contraindications, and complications; and interpreting their results: Advanced cardiac life support Abdominal paracentesis Arterial puncture Arthrocentesis Central venous line placement Lumbar puncture Nasogastric intubation Pap smear and endocervical culture Thoracentesis B. interpreting electrocardiograms.
34. How do I aspirate a joint?
Procedures Required for Certification in Internal Medicine For certification in internal medicine, the ABIM requires that candidates must be judged competent by their program directors in: A. performing the following procedures; understanding their indications, limitations, contraindications, and complications; and interpreting their results: Advanced cardiac life support Abdominal paracentesis Arterial puncture Arthrocentesis Central venous line placement Lumbar puncture Nasogastric intubation Pap smear and endocervical culture Thoracentesis B. interpreting electrocardiograms.
35. Guide to aspirating a joint
EQUIPMENT: Iodine for cleaning Gauze 2cc 2% lidocaine 10cc syringes 20 G (YELLOW) needles for aspirating (sometimes 18g if lots of pus, 22g if small joint), 25 G (BROWN) for anesthetic clean vacutainer tubes � 1 red top 1 purple top. Lots of alcohol wipes Band-aid
NEJM knee aspiration video37. What to do with the fluid
Samples for: Cell count (purple top) Gram Stain (red-top) Culture (red-top) No need to innoculate into blood culture bottles Clean top of tube to reduce contaminants 1.5% of organisms grown are contaminants. Crystals (red-top) Odd stuff in special circumstances: AFB stain and culture Fungal stain and culture Glucose � if low suggests infection
38. SYNOVIAL FLUID ANALYSIS
39. ADDITIONAL TESTS
X-ray Rule out osteomyelitis Establish baseline Changes take several weeks to develop ESR/CRP Blood cultures UA and Culture
40. What happens in the joint?
Direct Bacterial Bacteria deposit in the synovium Absence of basement membrane, therefore bacterial organisms enter the synovial fluid S. aureus binds to intra-articular proteins through adhesin proteins, and release chondrocyte proteases Inflammatory Response Mechanism Cytokine release causes hydrolysis of collagen and proteoglycans Tissue Ischemia Large effusions cause pressure necrosis and cartilage anoxia Degree of arthritis depends on presence or absence of these superantigens. Degree of arthritis depends on presence or absence of these superantigens.
41. EMPIRIC TREATMENT
Serial aspiration until dry tap Check GS, Culture and WCC on every sample to check clearing Immobilize joint for first 2 days Passive range of motion after first 2 days Active range of motion/weight bearing as resolving Start PT early to preserve ROM
42. WHEN TO CALL ORTHOPEDICS
JOINTS THAT CANNOT BE ASPIRATED AT BEDSIDE Hip joints Sacroiliac Prosthetic OTHER Osteomyelitis Unable to aspirate because fluid loculated Failing to respond Persistent positive cultures Failure of WBC to decrease Delayed onset of therapy >7 days Irreversible cartilage damage starts within 1 week
43. IVDA
Staph. aureus most common Also gram negatives Pseudomonas Serratia Insidious onset Propensity for axial skeleton Lumbar vertebrae Sacroiliacs Symphysis pubis Ischium Sternocostal joints Do well unless they have HIV
44. PROSTHETIC JOINTS
Overall infection rate 1% Revision arthroplasty 5-10% ORGANISMS: Early (6-12mths): Staph. epidermidis Late (>12mths): Staph. aureus Organisms seed the polysaccharide mucoid biofilm PRESENTATION: Early: pain, swelling, fever, drainage Late: indolent joint pain, <50% have fever and <10% have leukocytosis Bone scan shows increased uptake around prosthesis MANAGEMENT Surgical removal. Add rifampin Morality 5-20%
45. PROGNOSIS
5-15% mortality Co-morbidities contribute to mortality e.g. endocarditis, RA, sepsis, hemodialysis 30-50% of patients have residual damage to joint POOR PROGNOSTIC FACTORS: RA Delayed diagnosis Polyarticular sepsis Immunosuppressive therapy Positive blood cultures Gram negative organisms Elderly Renal transplant/dialysis
46. DIFFERENTIAL
Gout and Pseudogout (aka �pseudosepsis�) Bursitis RA Usually symmetrical polyarthritis Lyme Monoarthritis weeks or months after infection Viral arthritis Parvovirus: Small joints symmetric polyarthritis Reactive arthritis Prior GI/GU symptoms, conjunctivitis, skin rashes Rheumatic fever Large joint oligoarthritis �palindromic Jones criteria � Joints, Heart, Nodules, Erythema marginatum, Chorea
47. CASE
A 52 year old male carpenter presents to you with swelling of his elbow. On examination he has a full range of flexion, extension, pronation and supination but has a large swelling over the olecranon What is the DDX and how should he be treated?
48. CASE
A 52 year old male carpenter presents to you with swelling of his elbow. On examination he has a full range of flexion, extension, pronation and supination but has a large swelling over the olecranon What is the DDX and how should he be treated?
49. Septic bursitis
Usually olecranon and pre-patellar bursa Abrupt onset of pain swelling and erythema Transcutaneous entry trauma to skin eg. Carpenters 50% have associated cellulitis 80% due to Staph. aureus Blood cultures often negative Management Aspirate bursa Intravenous antibiotics
50. PROCEDURE
Find your landmarks Place a mark with the tip of a pen Clean with iodine Lidocaine sq 1-2cc of 2% (*the more the merrier � makes your and the pts life easier*) Wait 1 minute�� Aspirate with 20 g. Band-Aid
51. SUMMARY
In young healthy adults think of GC Most septic arthritis is due to Staph. aureus In IVDA consider gram negatives. Lupus and Hbopathies consider salmonella. If polyarticular septic arthritis likely seeding from endocarditis If the joint moves well but there is swelling and erythema it may be bursitis.