Download
1 / 17
180 likes | 1.82k Views
Clinical Information: Patient is a 70y/o female who is on prednisone for arthritis and presents with recent onset of cough. CXR shows prominent interstitial markings. Patient is a 54y/o female who had an interstitial pattern on CXR. Differential diagnosis. Sarcoid Langerhans Idiopathic

E N D
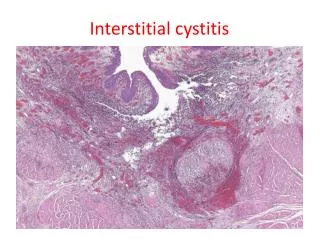
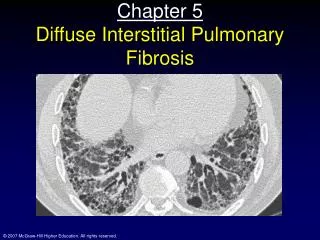
Clinical Information:Patient is a 70y/o female who is on prednisone for arthritis and presents with recent onset of cough. CXR shows prominent interstitial markings.
Patient is a 54y/o female who had an interstitial pattern on CXR.
Differential diagnosis Sarcoid Langerhans Idiopathic Desquamative Coal workers Bagassosis Silicosis Drug reaction Asbestosis Lymphangitic Erdheim Chester Lymphangiomyomatosis Chronic failure Farmer’s lung AnkylosingSpondylitis Neurofibromatosis Rheumatoid Scleroderma Hard metal disease Emphysema PAP Aspiration Gauchers Sjogrens LIP Mushroom workers lung Methotrexate lung Respiratory bronchiolitis BOOP Periarteritisnodosa Lupus Bronchiectasis Berylliosis Bronchiolitisobliterans Alveolar microlithiasis Metastatic calcification
Differential diagnosis More than 100 entities manifest as diffuse lung disease. Fortunately only 10-20 of these account for about 90% of all diffuse lung disease that is assessed by open lung biopsy. Sarcoid Langerhans granulomatosis Idiopathic pulmonary fibrosis Lymphangitic tumor Edema Asbestosis Collagen vascular diseases Silicosis Farmer’s lung Drugs
Differential diagnosis HONEYCOMBING & BRONCHIECTASIS Pulmonary fibrosis (IPF, RA, scleroderma, drug reaction, asbestosis, end-stage hypersensitivity pneumonitis) Sarcoidosis BRONCHIECTASIS Sarcoidosis Pulmonary fibrosis Hypersensitivity pneumonitis Allergic bronchopulmonaryaspergilosis Cystic fibrosis MOSAIC ATTENUATION BronchiolitisObliterans Cystic fibrosis Chronic PE AIR TRAPPING Obliterativebronchiolitis Asthma Hypersensitivity pneumonitis Normal variant (seen in superior segement of left lobe, middle lobe or lingula) NODULAR SEPTAL THICKENING, HONEYCOMBING & BRONCHIECTASIS Idiopathic pulmonary fibrosis Sarcoidosis (end-stage)
Diagnosis Pulmonary Fibrosis associated with Rheumatoid Arthritis
Information from literature “Diseases such as rheumatoid arthritis and scleroderma are also associated with diffuse interstitial thickening. Pathologically, there may be a UIP or NSIP pattern, indistinguishable from IPF. Dyspnea is a common complaint. Prognosis is variable and life-expectancy is longer with NSIP than UIP.” Practical Approach HRCT Jud W Gurney MD FACR Charles A Dobry Professor of Radiology University of Nebraska
Rheumatoid Arthritis Thoracic involvement often develops in patients as their disease progresses. Pleural disease is the most common thoracic manifestation. Pleural thickening is the next most common finding and is seen more often than pleural effusion. Pleural effusions are usually unilateral and may be loculated. Pulmonary fibrosis occurs in 2%–9% of patients with rheumatoid arthritis. High-resolution CT scans show a reticular pattern and irregular interlobular septal thickening predominantly in the lung periphery and lower lung zones Honeycombing and progressive volume loss develop as the disease progresses. In rare cases, fibrosis may be limited to the upper lobes and contain areas of cavitation, characteristics that mimic those of tuberculosis. Like any patient with pulmonary fibrosis, patients with pulmonary fibrosis associated with rheumatoid arthritis have an increased prevalence of lung cancer. RadioGraphics 2000; 20:1623–1635
Rheumatoid Arthritis Pulmonary nodules are uncommon in patients with rheumatoid arthritis and are usually associated with advanced disease and subcutaneous nodules. Usually multiple and well circumscribed, they often result in thick walled cavities. Patients with RA have an increased prevalence of airway diseases such as bronchiolitis obliterans and BOOP. Obliterative bronchiolitis occurs with increased frequency in patients with rheumatoid arthritis regardless of whether they have received penicillamine or gold therapy. HRCT may show a characteristic mosaic pattern of attenuation and perfusion. The predominant radiographic and high-resolution CT finding in patients with BOOP is airspace consolidation that is usually bilateral and tends to have a patchy peripheral or peribronchial distribution. RadioGraphics 2000; 20:1623–1635